S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
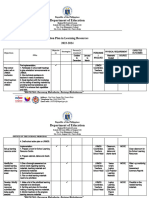
- aCTION PLAN IN HEALTHDocument13 paginiaCTION PLAN IN HEALTHCATHERINE FAJARDOÎncă nu există evaluări
- Adjectives Weekly Plan1Document10 paginiAdjectives Weekly Plan1RItta MariaÎncă nu există evaluări
- How To Retract BPS Data Back To R3 When There Is No Standard RetractorDocument3 paginiHow To Retract BPS Data Back To R3 When There Is No Standard Retractorraphavega2010Încă nu există evaluări
- Inventory of Vacant Units in Elan Miracle Sector-84 GurgaonDocument2 paginiInventory of Vacant Units in Elan Miracle Sector-84 GurgaonBharat SadanaÎncă nu există evaluări
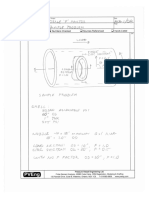
- Nozzle F Factor CalculationsDocument5 paginiNozzle F Factor CalculationsSivateja NallamothuÎncă nu există evaluări
- What Is Gross Income - Definition, Formula, Calculation, and ExampleDocument7 paginiWhat Is Gross Income - Definition, Formula, Calculation, and ExampleKapil SharmaÎncă nu există evaluări
- 1989 Volvo 740 Instruments and ControlsDocument107 pagini1989 Volvo 740 Instruments and Controlsskyliner538Încă nu există evaluări
- Optra - NubiraDocument37 paginiOptra - NubiraDaniel Castillo PeñaÎncă nu există evaluări
- Iso 16399-2014-05Document52 paginiIso 16399-2014-05nadim100% (1)
- Determination of Salicylic Acid'S Level in Acne Cream Which Sold in Kemiling Using Spektrofotmetry Uv VisDocument7 paginiDetermination of Salicylic Acid'S Level in Acne Cream Which Sold in Kemiling Using Spektrofotmetry Uv VisJuan LambeyÎncă nu există evaluări
- Adjective: the girl is beautifulDocument15 paginiAdjective: the girl is beautifulIn'am TraboulsiÎncă nu există evaluări
- Duet Embedded Memories and Logic Libraries For TSMC 28HP: HighlightsDocument5 paginiDuet Embedded Memories and Logic Libraries For TSMC 28HP: HighlightsmanojkumarÎncă nu există evaluări
- TheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesDocument1 paginăTheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesImpulsive collectorÎncă nu există evaluări
- Instruction Manual PC Interface RSM 100: TOSHIBA Corporation 1999 All Rights ReservedDocument173 paginiInstruction Manual PC Interface RSM 100: TOSHIBA Corporation 1999 All Rights ReservedFarid HakikiÎncă nu există evaluări
- Trend Graphs - Sample AnswerDocument4 paginiTrend Graphs - Sample AnswerannieannsÎncă nu există evaluări
- A Secret Baby by The Bratva by Lexi AsherDocument184 paginiA Secret Baby by The Bratva by Lexi Asheralisa sanchez100% (1)
- Case NoDocument13 paginiCase NoLaurente JessicaÎncă nu există evaluări
- 2-STM Answers SokhaDocument6 pagini2-STM Answers SokhamenghokcÎncă nu există evaluări
- Linear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisDocument11 paginiLinear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisPhD EEÎncă nu există evaluări
- DesignWS P1 PDFDocument673 paginiDesignWS P1 PDFcaubehamchoi6328Încă nu există evaluări
- Big Data, Consumer Analytics, and The Transformation of MarketingDocument17 paginiBig Data, Consumer Analytics, and The Transformation of MarketingPeyush NeneÎncă nu există evaluări
- Laptop repair messageDocument3 paginiLaptop repair messagePonpes Manbaul MaarifÎncă nu există evaluări
- Long Standoff Demolition Warheads For Armor, Masonry and Concrete TargetsDocument27 paginiLong Standoff Demolition Warheads For Armor, Masonry and Concrete Targetsahky7Încă nu există evaluări
- AP Biology Isopod LabDocument5 paginiAP Biology Isopod LabAhyyaÎncă nu există evaluări
- JMC250Document2 paginiJMC250abhijit99541623974426Încă nu există evaluări
- E Series CatalystDocument1 paginăE Series CatalystEmiZÎncă nu există evaluări
- Sine and Cosine Exam QuestionsDocument8 paginiSine and Cosine Exam QuestionsGamer Shabs100% (1)
- Water 07 02314Document36 paginiWater 07 02314Satyajit ShindeÎncă nu există evaluări
- Froyen06-The Keynesian System I - The Role of Aggregate DemandDocument40 paginiFroyen06-The Keynesian System I - The Role of Aggregate DemandUditi BiswasÎncă nu există evaluări
- Pneapple Waste To Bioethanol Casabar - Et - Al-2019-Biomass - Conversion - and - BiorefineryDocument6 paginiPneapple Waste To Bioethanol Casabar - Et - Al-2019-Biomass - Conversion - and - Biorefineryflorian willfortÎncă nu există evaluări