S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- ICDL Advanced Modules 01.05 PDFDocument1 paginăICDL Advanced Modules 01.05 PDFZICOÎncă nu există evaluări
- Short IIEF PDFDocument1 paginăShort IIEF PDFZICOÎncă nu există evaluări
- Medical Education in Egypt PDFDocument9 paginiMedical Education in Egypt PDFZICOÎncă nu există evaluări
- PHQ 9 en FRDocument3 paginiPHQ 9 en FRZICOÎncă nu există evaluări
- Robotic UrologyDocument279 paginiRobotic UrologyZICOÎncă nu există evaluări
- Lab Urine-AnalysisDocument6 paginiLab Urine-AnalysisZICOÎncă nu există evaluări
- Technical Solutions To Improve The Management of Non-muscle-Invasive Transitional Cell CarcinomaDocument42 paginiTechnical Solutions To Improve The Management of Non-muscle-Invasive Transitional Cell CarcinomaZICOÎncă nu există evaluări
- Male InfertilityDocument254 paginiMale InfertilityZICO100% (2)
- Premature EjaculationDocument381 paginiPremature EjaculationBarış Musa Tetik100% (3)
- Male Lower Urinary Tract Symptoms & Benign Prostatic HyperplasiaDocument106 paginiMale Lower Urinary Tract Symptoms & Benign Prostatic HyperplasiaZICO0% (1)
- Guidelines On: PriapismDocument30 paginiGuidelines On: PriapismZICOÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Good Surgical PracticeDocument16 paginiGood Surgical PracticedrdomengÎncă nu există evaluări
- Usaf Nurse Corps-Information Booklet-4feb13Document39 paginiUsaf Nurse Corps-Information Booklet-4feb13Jorge Vigoreaux100% (1)
- Nausea and Vomitting-FonDocument52 paginiNausea and Vomitting-FonZephas HillsÎncă nu există evaluări
- 2022 Draft H 2.2 General Hospitals Sections 1 2Document64 pagini2022 Draft H 2.2 General Hospitals Sections 1 2yasser dossokiÎncă nu există evaluări
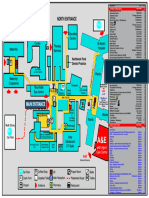
- Northwick Park Hospital Site MapDocument1 paginăNorthwick Park Hospital Site MapHasaan KhanÎncă nu există evaluări
- The Nature of A TermDocument6 paginiThe Nature of A TermJestril RacimoÎncă nu există evaluări
- Nur 460 Capstone Final PaperDocument15 paginiNur 460 Capstone Final Paperapi-429837528Încă nu există evaluări
- (B-0270) Day Surgery Procedure UnitDocument22 pagini(B-0270) Day Surgery Procedure UnitAhmad Gamal Elden MAhanyÎncă nu există evaluări
- National Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Document7 paginiNational Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Arnav JoshiÎncă nu există evaluări
- ReferatDocument23 paginiReferatmirantikaÎncă nu există evaluări
- The Impact of Internal Marketing On Service Quality, Perceived Value, Consumer Satisfaction and Loyalty in The Service SectorDocument10 paginiThe Impact of Internal Marketing On Service Quality, Perceived Value, Consumer Satisfaction and Loyalty in The Service SectorInternational Journal of Multidisciplinary Research and AnalysisÎncă nu există evaluări
- Essential Suite: BrochureDocument15 paginiEssential Suite: Brochuretempest8Încă nu există evaluări
- WONCA2013 - Book of Abstracts PDFDocument830 paginiWONCA2013 - Book of Abstracts PDFBruno ZanchettaÎncă nu există evaluări
- Chapter 12 - Patient Safety - APIC Text OnlineDocument30 paginiChapter 12 - Patient Safety - APIC Text OnlineManalAbdelazizÎncă nu există evaluări
- Gort No 2471Document8 paginiGort No 2471Abhishek DixitÎncă nu există evaluări
- Servier BrochureDocument42 paginiServier BrochureShuvam SehdevÎncă nu există evaluări
- Cancer Hospital and Reserach Center - Dissertation - SynopsisDocument3 paginiCancer Hospital and Reserach Center - Dissertation - SynopsisMeenu Abirami100% (1)
- Profile Services Design Process Projects Contact Us: IndiaDocument52 paginiProfile Services Design Process Projects Contact Us: Indiahasna.alamÎncă nu există evaluări
- Please Quote This Reference Number in All Future CorrespondenceDocument2 paginiPlease Quote This Reference Number in All Future CorrespondenceKrishna ManchiÎncă nu există evaluări
- AMA Journal of EthicsDocument83 paginiAMA Journal of EthicsOmarÎncă nu există evaluări
- Anxiety NCP - Anxiety - PatientDocument1 paginăAnxiety NCP - Anxiety - Patientnajm ktkÎncă nu există evaluări
- Uncertainty in MedicineDocument4 paginiUncertainty in MedicineShahidil SarilÎncă nu există evaluări
- NHS FPX 6008 Assessment 4 Lobbying For ChangeDocument4 paginiNHS FPX 6008 Assessment 4 Lobbying For ChangeEmma WatsonÎncă nu există evaluări
- Improving Nurse ResponsivenessDocument13 paginiImproving Nurse Responsivenessapi-446692943Încă nu există evaluări
- CLINICAL & MANAGERIAL KPIsDocument71 paginiCLINICAL & MANAGERIAL KPIsNatasha Bhasin100% (1)
- Energy Medicine For Today PDFDocument31 paginiEnergy Medicine For Today PDFshafiuthaÎncă nu există evaluări
- NursingAR 1011Document19 paginiNursingAR 1011Tatiana SiregarÎncă nu există evaluări
- Common Ethical Workplace Dilemmas: Taking Credit For Others' WorkDocument29 paginiCommon Ethical Workplace Dilemmas: Taking Credit For Others' WorkAshishMahajanÎncă nu există evaluări
- Heimeshof 2012 - Cost of Illness of Cystic FibrosisDocument15 paginiHeimeshof 2012 - Cost of Illness of Cystic FibrosisTri Purma SariÎncă nu există evaluări
- NPP Evaluation Case Study Report - The Spine Center at Dartmouth-HitchcockDocument7 paginiNPP Evaluation Case Study Report - The Spine Center at Dartmouth-HitchcockNikeshKumarSinghÎncă nu există evaluări