S-ar putea să vă placă și
- 4 5782675776138642694 PDFDocument1 pagină4 5782675776138642694 PDFNgh33Încă nu există evaluări
- Shanghairanking'S Global Ranking of Academic Subjects 2019 - Clinical MedicineDocument13 paginiShanghairanking'S Global Ranking of Academic Subjects 2019 - Clinical MedicineNgh33Încă nu există evaluări
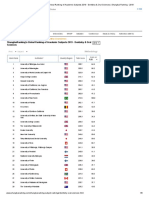
- Shanghairanking'S Global Ranking of Academic Subjects 2019 - Dentistry & Oral SciencesDocument8 paginiShanghairanking'S Global Ranking of Academic Subjects 2019 - Dentistry & Oral SciencesNgh33Încă nu există evaluări
- 2323 2329 Art. 3092 PDFDocument7 pagini2323 2329 Art. 3092 PDFNgh33Încă nu există evaluări
- Application For A Residence Permit in Denmark in Order To Obtain A Danish Authorisation or As A VolunteerDocument8 paginiApplication For A Residence Permit in Denmark in Order To Obtain A Danish Authorisation or As A VolunteerNgh33Încă nu există evaluări
- 10 1111@j 1468-3083 2012 04658 XDocument4 pagini10 1111@j 1468-3083 2012 04658 XNgh33Încă nu există evaluări
- Dentistry: (For International Students)Document2 paginiDentistry: (For International Students)Ngh33Încă nu există evaluări
- Gangadharan 2009Document11 paginiGangadharan 2009Ngh33Încă nu există evaluări
- Albietz 2006Document8 paginiAlbietz 2006Ngh33Încă nu există evaluări
- Nagy 2006Document11 paginiNagy 2006Ngh33Încă nu există evaluări
- Wong 2015Document3 paginiWong 2015Ngh33Încă nu există evaluări
- Darley 1982Document7 paginiDarley 1982Ngh33Încă nu există evaluări
- Torner 2016Document6 paginiTorner 2016Ngh33Încă nu există evaluări
- Torner 2016Document6 paginiTorner 2016Ngh33Încă nu există evaluări
- Gonzalez Iglesias2008Document10 paginiGonzalez Iglesias2008Ngh33Încă nu există evaluări
- Trisno 2015Document1 paginăTrisno 2015Ngh33Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- BEED 109 The Teaching of Edukasyong Pantahanan at Pangkabuhayan EPP-1Document13 paginiBEED 109 The Teaching of Edukasyong Pantahanan at Pangkabuhayan EPP-1CionbasÎncă nu există evaluări
- 3339 MT ReviewDocument6 pagini3339 MT ReviewNnaji DimiriÎncă nu există evaluări
- ANOVADocument3 paginiANOVAAbir HasanÎncă nu există evaluări
- A Linear Programming Optimization Approach To Costs Minimization in Port Terminal Operations in Nigerian PortsDocument6 paginiA Linear Programming Optimization Approach To Costs Minimization in Port Terminal Operations in Nigerian PortsInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- 2020 WIEMSPRO Wiemspro Effects of Whole-Body Electromyostimulation On Physical Fitness in Postmenopausal Women - A Randomized Controlled TrialDocument16 pagini2020 WIEMSPRO Wiemspro Effects of Whole-Body Electromyostimulation On Physical Fitness in Postmenopausal Women - A Randomized Controlled TrialVALERIO KIKUCHIÎncă nu există evaluări
- Theory Assessmentand Interventionof Academic ProcrastinationDocument45 paginiTheory Assessmentand Interventionof Academic ProcrastinationkeyzaÎncă nu există evaluări
- Adoption of Integrated Lean-Green-Agile Strategies For Modern Manufacturing SystemsDocument6 paginiAdoption of Integrated Lean-Green-Agile Strategies For Modern Manufacturing SystemsNuriaÎncă nu există evaluări
- Nursing Process in CommunityDocument8 paginiNursing Process in CommunityFahim Ahmed100% (1)
- Analysis On The Movie "Das Experiment"Document2 paginiAnalysis On The Movie "Das Experiment"Zeynep Çabuk100% (1)
- Deep Learning For Undersampled MRI ReconstructionDocument20 paginiDeep Learning For Undersampled MRI ReconstructionUsman KhalidÎncă nu există evaluări
- Motivation in Physical Activity Contexts: The Relationship of Perceived Motivational Climate To Intrinsic Motivation and Self-EfficacyDocument17 paginiMotivation in Physical Activity Contexts: The Relationship of Perceived Motivational Climate To Intrinsic Motivation and Self-EfficacyAndreea GligorÎncă nu există evaluări
- CV Kevin Ikhwan Muhammad Pt. Hasakona BinaciptaDocument6 paginiCV Kevin Ikhwan Muhammad Pt. Hasakona BinaciptaKevin MuhammadÎncă nu există evaluări
- Smu PM MB0050Document149 paginiSmu PM MB0050Sunilkumar DesarajuÎncă nu există evaluări
- Title of Project: Box 16. GAD Checklist For Project Management and ImplementationDocument7 paginiTitle of Project: Box 16. GAD Checklist For Project Management and ImplementationArniel Fred Tormis FernandezÎncă nu există evaluări
- Science, Technology, and The Future New Mentalities, NewDocument1 paginăScience, Technology, and The Future New Mentalities, NewSheena Racuya100% (1)
- E-HRM: Emerging HR Practices in Private Banks: ISSN (ONLINE) : 2250-0758, ISSN (PRINT) : 2394-6962Document6 paginiE-HRM: Emerging HR Practices in Private Banks: ISSN (ONLINE) : 2250-0758, ISSN (PRINT) : 2394-6962Ifthisam banuÎncă nu există evaluări
- Forrester - A Simple Prioritization ModelDocument4 paginiForrester - A Simple Prioritization ModelSalvador Vazquez OlimonÎncă nu există evaluări
- Curriculum Leadership Chapter 5Document15 paginiCurriculum Leadership Chapter 5JeyShidaÎncă nu există evaluări
- 6 SigmaDocument13 pagini6 SigmaThee BouyyÎncă nu există evaluări
- Distortional Buckling of CFS BeamsDocument404 paginiDistortional Buckling of CFS BeamsNazar BazaraaÎncă nu există evaluări
- CRM Master ThesisDocument4 paginiCRM Master Thesistracyberrycary100% (2)
- Software Engineering Lecture 2 - UpdatedDocument54 paginiSoftware Engineering Lecture 2 - UpdatedMuhammad ArslanÎncă nu există evaluări
- Jurnal - Paliatif - Rama-SuryaDocument4 paginiJurnal - Paliatif - Rama-SuryaRama Mikril JulyanaÎncă nu există evaluări
- Preventive Maintenance Strategies for Filling EquipmentDocument9 paginiPreventive Maintenance Strategies for Filling EquipmentmaulanahafishÎncă nu există evaluări
- Primary Data Are Those Which Are Collected Afresh and For The First Primary Data Are Those Which Are Collected Afresh and For The FirstDocument18 paginiPrimary Data Are Those Which Are Collected Afresh and For The First Primary Data Are Those Which Are Collected Afresh and For The FirstBhagawat SwaroopÎncă nu există evaluări
- How PISA Changed Global Education Standards and PerformanceDocument9 paginiHow PISA Changed Global Education Standards and PerformanceVelma ParungaoÎncă nu există evaluări
- Web-Based Bohol Cacao Industry DatabaseDocument7 paginiWeb-Based Bohol Cacao Industry DatabaseSheila GarciaÎncă nu există evaluări
- Bentuk Dan Ciri Adjektiva Bahasa Dayak Ngaju (Forms and Characteristics of Dayak Ngaju Language) Elisten Parulian SigiroDocument16 paginiBentuk Dan Ciri Adjektiva Bahasa Dayak Ngaju (Forms and Characteristics of Dayak Ngaju Language) Elisten Parulian SigiroNovitaÎncă nu există evaluări
- The Effect of Motivation On Organizational PerformanceDocument22 paginiThe Effect of Motivation On Organizational PerformanceZoraiz FazalÎncă nu există evaluări
- Factor Analysis Source Code AppendixDocument20 paginiFactor Analysis Source Code Appendixpratik zankeÎncă nu există evaluări