S-ar putea să vă placă și
- A Guide to District Court Civil Forms in the State of HawaiiDe la EverandA Guide to District Court Civil Forms in the State of HawaiiÎncă nu există evaluări
- Drug Test Request: Accession No.: OR#: Code No.Document6 paginiDrug Test Request: Accession No.: OR#: Code No.OptimaCare MalabonÎncă nu există evaluări
- Random Drug Test: CertificationDocument2 paginiRandom Drug Test: CertificationApril BoreresÎncă nu există evaluări
- Laboratory Procedure For Specimen HandlingDocument38 paginiLaboratory Procedure For Specimen HandlingGail IbanezÎncă nu există evaluări
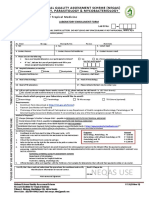
- NEQAS Enrollment Form V7.0 PDFDocument2 paginiNEQAS Enrollment Form V7.0 PDFMyline CampoamorÎncă nu există evaluări
- Immunization RecordDocument4 paginiImmunization RecordVin BitzÎncă nu există evaluări
- New Guidelines On The Issuance of Certificate of InclusionDocument7 paginiNew Guidelines On The Issuance of Certificate of InclusionRosanna Paulican100% (1)
- Application For Leave of AbsenceDocument1 paginăApplication For Leave of AbsenceTess Aboc100% (1)
- Title: Pregnancy Test Strip Pages: 5Document5 paginiTitle: Pregnancy Test Strip Pages: 5Gakwaya Jules CesarÎncă nu există evaluări
- 6.OPMS Discharge Permit Engr. Cherry BombalesDocument58 pagini6.OPMS Discharge Permit Engr. Cherry BombalesDyeri FloresÎncă nu există evaluări
- X RAY ResultsDocument1 paginăX RAY ResultsJaneÎncă nu există evaluări
- Doh DC 2018-0142Document2 paginiDoh DC 2018-0142vanceÎncă nu există evaluări
- 2020 NEQAS CC Registration Form and Order of PaymentDocument2 pagini2020 NEQAS CC Registration Form and Order of PaymentNovie FeneciosÎncă nu există evaluări
- Application Form Blood Collection Unit Blood StationDocument5 paginiApplication Form Blood Collection Unit Blood StationRhodora BenipayoÎncă nu există evaluări
- DTTB Hiring DeploymentDocument2 paginiDTTB Hiring DeploymentIsrael GoticoÎncă nu există evaluări
- Nkti NRLDocument1 paginăNkti NRLlaboratoryÎncă nu există evaluări
- Individual Performance Commitment and Review (Ipcr)Document2 paginiIndividual Performance Commitment and Review (Ipcr)Reuben Jr UmallaÎncă nu există evaluări
- 1.0 Functionality of The Local Health BoardDocument3 pagini1.0 Functionality of The Local Health BoardEivenn Panerio100% (2)
- PBCC PDFDocument1 paginăPBCC PDFMaureen Dela ResmaÎncă nu există evaluări
- ManufacturingDocument11 paginiManufacturingKitkat CasacopÎncă nu există evaluări
- Summary TQMDocument3 paginiSummary TQMAngelo Del Rosario50% (2)
- RITM Laboratory Diagnostic Services BrochureDocument65 paginiRITM Laboratory Diagnostic Services BrochureRITM DOH67% (3)
- DOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureDocument1 paginăDOH-HFSRB-QOP-01-Form 2 A: Print Name and SignatureJm Cayabyab0% (1)
- Hospital Blood Transfusion Committee ReportDocument3 paginiHospital Blood Transfusion Committee ReportCharmaine Corpuz Granil0% (1)
- Annex B Konsulta ChecklistDocument8 paginiAnnex B Konsulta ChecklistFret Ramirez Coronia RNÎncă nu există evaluări
- Resolution No. 22-022 Blood DonaitonDocument2 paginiResolution No. 22-022 Blood DonaitonDontogan BarangayÎncă nu există evaluări
- Authorization Letter For PRC TransactionDocument1 paginăAuthorization Letter For PRC TransactionJemjay Ar ToldoÎncă nu există evaluări
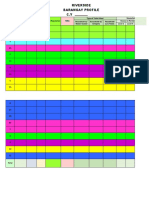
- Brgy Profile 2022Document6 paginiBrgy Profile 2022Louises Sayson-OlayanÎncă nu există evaluări
- RESOLUTIONSDocument4 paginiRESOLUTIONSjovelyn dahangÎncă nu există evaluări
- Blood Banking LawDocument50 paginiBlood Banking LawDayledaniel SorvetoÎncă nu există evaluări
- 06 Specimen Collection For HOL 2Document78 pagini06 Specimen Collection For HOL 2Irmina Fidelis Garcia100% (3)
- CPH FORM 2 - Common Household QuestionnaireDocument6 paginiCPH FORM 2 - Common Household Questionnairebanate LGU100% (1)
- PFC MatrixDocument48 paginiPFC Matrixjemma chayocasÎncă nu există evaluări
- ECC Request For ReliefDocument7 paginiECC Request For ReliefNoreen T� ClaroÎncă nu există evaluări
- Memo - Designation of Administrative StaffDocument1 paginăMemo - Designation of Administrative StaffRegion Personnel100% (1)
- Job Description of SDTL AnalystDocument4 paginiJob Description of SDTL AnalystCaesar A. AlesnaÎncă nu există evaluări
- Ao2019-0004.cut Off DatesDocument4 paginiAo2019-0004.cut Off DatesalissalvqsÎncă nu există evaluări
- Purchase Request Form 111Document3 paginiPurchase Request Form 111jay ar baybayÎncă nu există evaluări
- NEQAS Registration Form 2020-SerologyDocument2 paginiNEQAS Registration Form 2020-SerologyMark Jefferson Sanchez Merto100% (5)
- ABC Ref and Aircon SalesDocument5 paginiABC Ref and Aircon SalesLorilla AlvinÎncă nu există evaluări
- The Sangguniang Panlungsod: Panabo CityDocument3 paginiThe Sangguniang Panlungsod: Panabo CityVikki AmorioÎncă nu există evaluări
- Ipcr-Samillano, John Vanne D. Samillano, Rmt-Maayon RhuDocument5 paginiIpcr-Samillano, John Vanne D. Samillano, Rmt-Maayon RhuEdgar DumagpiÎncă nu există evaluări
- Self Monitoring Report System 1st Quarter 2015 2Document9 paginiSelf Monitoring Report System 1st Quarter 2015 2ARCHEMEDEZ RAMOSÎncă nu există evaluări
- Ihomis - HBSys OPD MODULE PDFDocument9 paginiIhomis - HBSys OPD MODULE PDFBads BrandaresÎncă nu există evaluări
- Certification: Office of The Punong BarangayDocument1 paginăCertification: Office of The Punong BarangayBarangay CatoÎncă nu există evaluări
- Letter Request To BFPDocument2 paginiLetter Request To BFPPaciano CansingÎncă nu există evaluări
- Administrative Orders of Ra 4688Document40 paginiAdministrative Orders of Ra 4688Joshua BacunawaÎncă nu există evaluări
- Assessment Tool For Accreditation of Drug Testing LaboratoryDocument8 paginiAssessment Tool For Accreditation of Drug Testing Laboratoryhealthpro diagnosticÎncă nu există evaluări
- Kato-Katz Method: LAVALLE, Jestin BDocument2 paginiKato-Katz Method: LAVALLE, Jestin BDixie DumagpiÎncă nu există evaluări
- Manual of Standards & Criteria For Lab Action Plan Ver 4.0 19 Nov 2015 (NHLN TWG 2015)Document18 paginiManual of Standards & Criteria For Lab Action Plan Ver 4.0 19 Nov 2015 (NHLN TWG 2015)Mic MostalesÎncă nu există evaluări
- Sop Drug Test LMMDocument35 paginiSop Drug Test LMMTalon General Hospital Laboratory Department100% (2)
- 8 RA 4688 (Clinical Laboratory Law)Document32 pagini8 RA 4688 (Clinical Laboratory Law)AIRRA CLAIRE ALVAREZÎncă nu există evaluări
- Application Form: Philippine Registry For Persons With Disabilities Version 4.0Document5 paginiApplication Form: Philippine Registry For Persons With Disabilities Version 4.0ANNA MARY GINTOROÎncă nu există evaluări
- CBMIS Barangay Tally SheetDocument4 paginiCBMIS Barangay Tally SheetShu ShuÎncă nu există evaluări
- PNSDWDocument35 paginiPNSDWpj100% (1)
- LWUA Tariff Setting For Septage ManagementDocument16 paginiLWUA Tariff Setting For Septage Managementchristine guardeÎncă nu există evaluări
- Medical Certificate Jean TamayoDocument5 paginiMedical Certificate Jean TamayoAugust Cherry MabbyÎncă nu există evaluări
- Pharmacists 04-2023Document17 paginiPharmacists 04-2023PRC BaguioÎncă nu există evaluări
- Official Receipt or Reference Number:: CertificationDocument3 paginiOfficial Receipt or Reference Number:: CertificationKhelly EspinoÎncă nu există evaluări
- Aperiomics Order Form: Xplore-PATHODocument2 paginiAperiomics Order Form: Xplore-PATHOSasu AlexandruÎncă nu există evaluări
- PAMET New Membership FormDocument1 paginăPAMET New Membership FormRitz Bautista BalanayÎncă nu există evaluări
- 01 Application (Permit To Construct)Document1 pagină01 Application (Permit To Construct)jherica baltazar100% (1)
- Brylle and Renz RecallsDocument11 paginiBrylle and Renz RecallsRitz Bautista Balanay100% (1)
- Recalls 4Document1 paginăRecalls 4Ritz Bautista BalanayÎncă nu există evaluări
- CoC & CCF Forms PDFDocument6 paginiCoC & CCF Forms PDFRitz Bautista BalanayÎncă nu există evaluări
- Recalls 4Document1 paginăRecalls 4Ritz Bautista BalanayÎncă nu există evaluări
- Brylle and Renz RecallsDocument11 paginiBrylle and Renz RecallsRitz Bautista Balanay100% (1)
- Checklist For Review of Floor Plans Drug Testing Laboratory 2017 PDFDocument2 paginiChecklist For Review of Floor Plans Drug Testing Laboratory 2017 PDFRitz Bautista Balanay100% (1)
- Tabrez Ahmad TPDocument33 paginiTabrez Ahmad TPGunjeet SinghÎncă nu există evaluări
- Tumino, Melissa AnneDocument4 paginiTumino, Melissa AnneJames LindonÎncă nu există evaluări
- Felons and RattlesnakesDocument3 paginiFelons and Rattlesnakesapi-462772385Încă nu există evaluări
- Mens ReaDocument30 paginiMens ReaedhaÎncă nu există evaluări
- United States v. Javonne Wilks, 464 F.3d 1240, 11th Cir. (2006)Document6 paginiUnited States v. Javonne Wilks, 464 F.3d 1240, 11th Cir. (2006)Scribd Government DocsÎncă nu există evaluări
- People Vs WongDocument2 paginiPeople Vs WongTukne SanzÎncă nu există evaluări
- (2a) TheftDocument12 pagini(2a) ThefthazzuÎncă nu există evaluări
- Article On Section 305 CRPCDocument4 paginiArticle On Section 305 CRPCLatest Laws TeamÎncă nu există evaluări
- 2020 HSC Legal StudiesDocument24 pagini2020 HSC Legal StudiesLÎncă nu există evaluări
- Launch Trampoline Park WaiverDocument1 paginăLaunch Trampoline Park WaiverGabrielle Glass-HardingÎncă nu există evaluări
- 9 Sagrada Orden Vs NACOCODocument1 pagină9 Sagrada Orden Vs NACOCOluigimanzanaresÎncă nu există evaluări
- Last Pleading On Criminal Law PrivacyDocument25 paginiLast Pleading On Criminal Law PrivacyEBY Traders100% (1)
- United States v. Nicholas Hincapie, 66 F.3d 551, 2d Cir. (1995)Document4 paginiUnited States v. Nicholas Hincapie, 66 F.3d 551, 2d Cir. (1995)Scribd Government DocsÎncă nu există evaluări
- Dizon Pamintuan vs. PeopleDocument6 paginiDizon Pamintuan vs. PeopleredrouxÎncă nu există evaluări
- Torts and Damages Midterm ReviewerDocument25 paginiTorts and Damages Midterm ReviewerErika-Anne ThereseÎncă nu există evaluări
- People vs. Ortega, G.R. No. 116736, July 24, 1997, 276 SCRA 166Document2 paginiPeople vs. Ortega, G.R. No. 116736, July 24, 1997, 276 SCRA 166Teoti Navarro Reyes100% (3)
- Agpalo Construction Notes Cases and Legal MaximsDocument19 paginiAgpalo Construction Notes Cases and Legal MaximsAnonymous o9q5eawTÎncă nu există evaluări
- RA 8048 - Coconut Preservation ActDocument3 paginiRA 8048 - Coconut Preservation Actskylark74Încă nu există evaluări
- 2012 Criminal Law Summer Reviewer - Book2 - MLWDocument167 pagini2012 Criminal Law Summer Reviewer - Book2 - MLWYla ParasÎncă nu există evaluări
- Aggravating & Mitigating FactorsDocument4 paginiAggravating & Mitigating FactorsMuhammad Amjad RafiqÎncă nu există evaluări
- CUMcv 05 313Document9 paginiCUMcv 05 313Chris BuckÎncă nu există evaluări
- Ranganathllb Legal NoticeDocument3 paginiRanganathllb Legal NoticeLatharani NPÎncă nu există evaluări
- Tort Law LecturesDocument235 paginiTort Law LecturesNavin SoborunÎncă nu există evaluări
- Federal District Court Trade Secret RulingDocument37 paginiFederal District Court Trade Secret RulingDaniel BallardÎncă nu există evaluări
- Letter To Fredericton Police Chief Barry MacKnightDocument2 paginiLetter To Fredericton Police Chief Barry MacKnightmchardieÎncă nu există evaluări
- People vs. TeeDocument2 paginiPeople vs. TeeVin LacsieÎncă nu există evaluări
- Shire Development Inc. v. Cadila Healthcare Limited (D/b/a Zydus Cadila), C.A. No. 10-581-KAJ (D. Del. Oct. 19, 2012)Document3 paginiShire Development Inc. v. Cadila Healthcare Limited (D/b/a Zydus Cadila), C.A. No. 10-581-KAJ (D. Del. Oct. 19, 2012)YCSTBlogÎncă nu există evaluări
- Carillo's Slides Reviewer For Pre-FiDocument15 paginiCarillo's Slides Reviewer For Pre-FiMary LeandaÎncă nu există evaluări
- 310-Cv-03647-WHA Docket 50 Notice of Voluntary Dismissal Without PrejudiceDocument2 pagini310-Cv-03647-WHA Docket 50 Notice of Voluntary Dismissal Without PrejudiceJ DoeÎncă nu există evaluări
- BRAZILDocument14 paginiBRAZILJericho ReyÎncă nu există evaluări
- Broken: The most shocking childhood story ever told. An inspirational author who survived it.De la EverandBroken: The most shocking childhood story ever told. An inspirational author who survived it.Evaluare: 5 din 5 stele5/5 (45)
- If You Tell: A True Story of Murder, Family Secrets, and the Unbreakable Bond of SisterhoodDe la EverandIf You Tell: A True Story of Murder, Family Secrets, and the Unbreakable Bond of SisterhoodEvaluare: 4.5 din 5 stele4.5/5 (1798)
- The Bigamist: The True Story of a Husband's Ultimate BetrayalDe la EverandThe Bigamist: The True Story of a Husband's Ultimate BetrayalEvaluare: 4.5 din 5 stele4.5/5 (104)
- The Girls Are Gone: The True Story of Two Sisters Who Vanished, the Father Who Kept Searching, and the Adults Who Conspired to Keep the Truth HiddenDe la EverandThe Girls Are Gone: The True Story of Two Sisters Who Vanished, the Father Who Kept Searching, and the Adults Who Conspired to Keep the Truth HiddenEvaluare: 3.5 din 5 stele3.5/5 (36)
- Selling the Dream: The Billion-Dollar Industry Bankrupting AmericansDe la EverandSelling the Dream: The Billion-Dollar Industry Bankrupting AmericansEvaluare: 4 din 5 stele4/5 (17)
- Hell Put to Shame: The 1921 Murder Farm Massacre and the Horror of America's Second SlaveryDe la EverandHell Put to Shame: The 1921 Murder Farm Massacre and the Horror of America's Second SlaveryEvaluare: 2.5 din 5 stele2.5/5 (3)
- Tinseltown: Murder, Morphine, and Madness at the Dawn of HollywoodDe la EverandTinseltown: Murder, Morphine, and Madness at the Dawn of HollywoodÎncă nu există evaluări
- Altamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayDe la EverandAltamont: The Rolling Stones, the Hells Angels, and the Inside Story of Rock's Darkest DayEvaluare: 4 din 5 stele4/5 (25)
- Perfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthDe la EverandPerfect Murder, Perfect Town: The Uncensored Story of the JonBenet Murder and the Grand Jury's Search for the TruthEvaluare: 3.5 din 5 stele3.5/5 (68)
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIDe la EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIEvaluare: 4 din 5 stele4/5 (19)
- Restless Souls: The Sharon Tate Family's Account of Stardom, the Manson Murders, and a Crusade for JusticeDe la EverandRestless Souls: The Sharon Tate Family's Account of Stardom, the Manson Murders, and a Crusade for JusticeÎncă nu există evaluări
- Double Lives: True Tales of the Criminals Next DoorDe la EverandDouble Lives: True Tales of the Criminals Next DoorEvaluare: 4 din 5 stele4/5 (34)
- Bind, Torture, Kill: The Inside Story of BTK, the Serial Killer Next DoorDe la EverandBind, Torture, Kill: The Inside Story of BTK, the Serial Killer Next DoorEvaluare: 3.5 din 5 stele3.5/5 (77)
- Witness: For the Prosecution of Scott PetersonDe la EverandWitness: For the Prosecution of Scott PetersonEvaluare: 3 din 5 stele3/5 (44)
- Nicole Brown Simpson: The Private Diary of a Life InterruptedDe la EverandNicole Brown Simpson: The Private Diary of a Life InterruptedEvaluare: 3.5 din 5 stele3.5/5 (16)
- The Rescue Artist: A True Story of Art, Thieves, and the Hunt for a Missing MasterpieceDe la EverandThe Rescue Artist: A True Story of Art, Thieves, and the Hunt for a Missing MasterpieceEvaluare: 4 din 5 stele4/5 (1)
- The Gardner Heist: The True Story of the World's Largest Unsolved Art TheftDe la EverandThe Gardner Heist: The True Story of the World's Largest Unsolved Art TheftÎncă nu există evaluări
- Bloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyDe la EverandBloodlines: The True Story of a Drug Cartel, the FBI, and the Battle for a Horse-Racing DynastyEvaluare: 4 din 5 stele4/5 (8)
- Diamond Doris: The True Story of the World's Most Notorious Jewel ThiefDe la EverandDiamond Doris: The True Story of the World's Most Notorious Jewel ThiefEvaluare: 3.5 din 5 stele3.5/5 (18)
- Cold-Blooded: A True Story of Love, Lies, Greed, and MurderDe la EverandCold-Blooded: A True Story of Love, Lies, Greed, and MurderEvaluare: 4 din 5 stele4/5 (53)
- Gotti's Rules: The Story of John Alite, Junior Gotti, and the Demise of the American MafiaDe la EverandGotti's Rules: The Story of John Alite, Junior Gotti, and the Demise of the American MafiaÎncă nu există evaluări
- Unanswered Cries: A True Story of Friends, Neighbors, and Murder in a Small TownDe la EverandUnanswered Cries: A True Story of Friends, Neighbors, and Murder in a Small TownEvaluare: 4.5 din 5 stele4.5/5 (179)
- Blood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyDe la EverandBlood Brother: 33 Reasons My Brother Scott Peterson Is GuiltyEvaluare: 3 din 5 stele3/5 (57)
- A Special Place In Hell: The World's Most Depraved Serial KillersDe la EverandA Special Place In Hell: The World's Most Depraved Serial KillersEvaluare: 4 din 5 stele4/5 (53)