S-ar putea să vă placă și
- Cardiovascular Physiology by Dr. Sana Bashir MS-CPPT, DPTDocument42 paginiCardiovascular Physiology by Dr. Sana Bashir MS-CPPT, DPTbkdfiesefllÎncă nu există evaluări
- The Circulatory System: The Heart, Blood Vessels, Blood TypesDocument51 paginiThe Circulatory System: The Heart, Blood Vessels, Blood TypesClemente Castañeda MontillaÎncă nu există evaluări
- The Circulatory System: The Heart, Blood Vessels, Blood TypesDocument51 paginiThe Circulatory System: The Heart, Blood Vessels, Blood Typescut irnandaÎncă nu există evaluări
- The Circulatory System: The Heart, Blood Vessels, Blood TypesDocument51 paginiThe Circulatory System: The Heart, Blood Vessels, Blood Typesghisma ocvintiaÎncă nu există evaluări
- The Circulatory System ExplainedDocument51 paginiThe Circulatory System ExplainedJonalynCollodChewacheoÎncă nu există evaluări
- 10 General Anatomy of The Cardiovascular SystemDocument140 pagini10 General Anatomy of The Cardiovascular SystemSuzana VoiculescuÎncă nu există evaluări
- Circulatory System: Heart, Blood Vessels & TypesDocument51 paginiCirculatory System: Heart, Blood Vessels & TypesTina TalmadgeÎncă nu există evaluări
- NCM 103-Cardio Anatomy & PhysioDocument56 paginiNCM 103-Cardio Anatomy & Physiolouradel100% (1)
- BLG111_Week2_Blood_Heart_2Document74 paginiBLG111_Week2_Blood_Heart_2phuongphuonganhanh171203Încă nu există evaluări
- Cardiac Anatomy and Physiology: Leaugeay Webre BS, CCEMT-P, Nremt-PDocument145 paginiCardiac Anatomy and Physiology: Leaugeay Webre BS, CCEMT-P, Nremt-Pa.abdullah.2005.111Încă nu există evaluări
- Cardiovascular SystemDocument93 paginiCardiovascular SystemMaria AlcantarÎncă nu există evaluări
- WK 1& 2 LectureDocument149 paginiWK 1& 2 LectureElma SekikorolevuÎncă nu există evaluări
- Anatomi-Fisiologi Psik Wo EcgDocument143 paginiAnatomi-Fisiologi Psik Wo EcgFidyalestariputriÎncă nu există evaluări
- Cardiovascular and Circulatory FunctionDocument271 paginiCardiovascular and Circulatory FunctionARAGON GEMMA LYNÎncă nu există evaluări
- Read 1 CVS OrgDocument34 paginiRead 1 CVS OrgEzeudu SomtoÎncă nu există evaluări
- Cardiovascular System: Claire R. Hatton, RN, MANDocument63 paginiCardiovascular System: Claire R. Hatton, RN, MANrhimineecat71Încă nu există evaluări
- Life's Progression Through Cardiac PhysiologyDocument91 paginiLife's Progression Through Cardiac PhysiologyprofcarleyÎncă nu există evaluări
- Cardiovascular DisordersDocument9 paginiCardiovascular Disordersdlneisha6175% (4)
- Circulatory System GuideDocument29 paginiCirculatory System GuideFerry SofatÎncă nu există evaluări
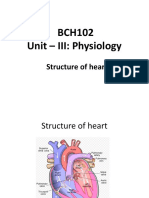
- Structure of the HeartDocument17 paginiStructure of the Heartdivya vajpayeeÎncă nu există evaluări
- Anatomy & Physiology Training OverviewDocument50 paginiAnatomy & Physiology Training OverviewAlisa BrownÎncă nu există evaluări
- Heart Blood HistoDocument53 paginiHeart Blood HistoAnonymous 52lBinÎncă nu există evaluări
- Cardiovascular System Study SheetDocument8 paginiCardiovascular System Study SheetTkÎncă nu există evaluări
- 07 - Cardiovascular System DeclutteredDocument54 pagini07 - Cardiovascular System DeclutteredFRANCINE JANE PATI�OÎncă nu există evaluări
- Simple Nursing Medical Surgical - CompletoDocument157 paginiSimple Nursing Medical Surgical - CompletoRenato Bandeira100% (4)
- Biology IGCSE Human Circulatory SystemDocument17 paginiBiology IGCSE Human Circulatory SystemNiharika100% (1)
- Cardiovascular Physiology: For HO StudentsDocument77 paginiCardiovascular Physiology: For HO StudentsMengistu GebeyehuÎncă nu există evaluări
- AbhiDocument16 paginiAbhiAkash VigneshwarÎncă nu există evaluări
- CVS & HypertensionDocument92 paginiCVS & HypertensionNimesh ModiÎncă nu există evaluări
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocument27 paginiCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3Încă nu există evaluări
- @PPT - Fisiologi Jantung - KD 2012Document70 pagini@PPT - Fisiologi Jantung - KD 2012irmayanti adewarjaÎncă nu există evaluări
- Cardionursing 110207023802 Phpapp01Document18 paginiCardionursing 110207023802 Phpapp01arvinnnnÎncă nu există evaluări
- Conducting System of The HeartDocument27 paginiConducting System of The HeartMuhammadÎncă nu există evaluări
- Day 7 Cardiac Perfussion Coronaria - KoronerDocument38 paginiDay 7 Cardiac Perfussion Coronaria - KoronerNiluh Putu NurindahÎncă nu există evaluări
- Cardiology Course Outline on Functional Anatomy and PhysiologyDocument19 paginiCardiology Course Outline on Functional Anatomy and PhysiologyImraan MohaÎncă nu există evaluări
- Cardiovascular System Anatomy and PhysiologyDocument24 paginiCardiovascular System Anatomy and PhysiologyAngela Christian TiczonÎncă nu există evaluări
- Cadiac Cycle, Heart Sound, ECG, HypertensionDocument110 paginiCadiac Cycle, Heart Sound, ECG, HypertensionNilesh100% (1)
- Cardiovascular System The HeartDocument38 paginiCardiovascular System The HearteliseudesafateÎncă nu există evaluări
- Components of The Cardiovascular SystemDocument23 paginiComponents of The Cardiovascular SystemMr. DummyÎncă nu există evaluări
- Cardiovascular Physical TherapyDocument206 paginiCardiovascular Physical TherapyJuanitoCabatañaLimIII100% (2)
- Cardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariDocument42 paginiCardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariAyu PuspitaÎncă nu există evaluări
- Anatomi Fisiologi Sistem Kardiovaskuler 1Document52 paginiAnatomi Fisiologi Sistem Kardiovaskuler 1Vaweli Putri Spelman DpÎncă nu există evaluări
- Cardiovascular System: by DR Saad ZafarDocument154 paginiCardiovascular System: by DR Saad Zafarkhalidtalal8000Încă nu există evaluări
- 1.1 CV PhysiologyDocument34 pagini1.1 CV PhysiologygilangbpÎncă nu există evaluări
- Anatomi Fisiology Sist - KV@DR - ZainiDocument46 paginiAnatomi Fisiology Sist - KV@DR - ZainiDikdik Iskandar DwiyantoÎncă nu există evaluări
- Circulatory SystemDocument56 paginiCirculatory SystemillyaniÎncă nu există evaluări
- Cardiology Ebook Notes PDFDocument26 paginiCardiology Ebook Notes PDFsugisweÎncă nu există evaluări
- Cardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPDocument90 paginiCardiac Anatomy and Physiology: Iris Ken R. Rico, OTRPAndra HijratulÎncă nu există evaluări
- Midterm, Circulatory System-Heart. PPT 15Document38 paginiMidterm, Circulatory System-Heart. PPT 15Lindley PareñoÎncă nu există evaluări
- CARDIOVASCULAR DISORDERS (CVD) OoDocument367 paginiCARDIOVASCULAR DISORDERS (CVD) OoMercy KeruboÎncă nu există evaluări
- Circulation: Ulysses John P. Almocera, RN, EMTDocument31 paginiCirculation: Ulysses John P. Almocera, RN, EMTCarlo SorinoÎncă nu există evaluări
- Cardiovascular System Anatomy and PhysiologyDocument24 paginiCardiovascular System Anatomy and PhysiologyAngela Christian TiczonÎncă nu există evaluări
- Cardiovascular System (Our Presention)Document14 paginiCardiovascular System (Our Presention)RicaMisakiÎncă nu există evaluări
- Lecture 4 Properties of Myocardium and Cardiac Cycle 2020-2021Document43 paginiLecture 4 Properties of Myocardium and Cardiac Cycle 2020-2021badarbhai222Încă nu există evaluări
- K 29 Sirkulasi Koroner - CVS K29Document16 paginiK 29 Sirkulasi Koroner - CVS K29Jane Andrea Christiano DjianzonieÎncă nu există evaluări
- A Muscular Double Pump: The HeartDocument43 paginiA Muscular Double Pump: The HeartConeisa ConanÎncă nu există evaluări
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!De la EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Încă nu există evaluări
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisDe la EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisEvaluare: 5 din 5 stele5/5 (1)
- Beating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartDe la EverandBeating with Precision: The Science of Cardiology: Understand the Intricacies of the Human HeartÎncă nu există evaluări
- Recurrence of Simple Febrile Seizure Who Follows Intermittent Prophylaxis: A Comparative Study Between Clobazam and DiazepamDocument5 paginiRecurrence of Simple Febrile Seizure Who Follows Intermittent Prophylaxis: A Comparative Study Between Clobazam and DiazepamancillaagraynÎncă nu există evaluări
- Acute Diarrhea in Children ResearchDocument9 paginiAcute Diarrhea in Children Researchamirah sinumÎncă nu există evaluări
- Fluid Dss PKB - RsDocument39 paginiFluid Dss PKB - RsancillaagraynÎncă nu există evaluări
- Jurding 3 PDFDocument6 paginiJurding 3 PDFNadya Prima PutriÎncă nu există evaluări
- JurnalDocument6 paginiJurnalancillaagraynÎncă nu există evaluări
- Infeksi Dengue AnakDocument67 paginiInfeksi Dengue AnakancillaagraynÎncă nu există evaluări
- Modern Management of Traumatic Hemothorax 2167 1222 1000326Document5 paginiModern Management of Traumatic Hemothorax 2167 1222 1000326anon_12953532Încă nu există evaluări
- 2016 Article 167Document11 pagini2016 Article 167Anonymous L396Tj4Încă nu există evaluări
- Missing Person's Clothing and ID DetailsDocument14 paginiMissing Person's Clothing and ID DetailsancillaagraynÎncă nu există evaluări
- 99149246Document11 pagini99149246Retma Rosela NurkayantyÎncă nu există evaluări
- APA Draft Schizophrenia Treatment Guideline Dec2019 PDFDocument414 paginiAPA Draft Schizophrenia Treatment Guideline Dec2019 PDFFransiska Yuka JuliaÎncă nu există evaluări
- Urticaria and Angioedema - An Update On Classification and Pathogenesis PDFDocument14 paginiUrticaria and Angioedema - An Update On Classification and Pathogenesis PDFancillaagraynÎncă nu există evaluări
- Pediatric AnaphylaxisDocument19 paginiPediatric AnaphylaxisancillaagraynÎncă nu există evaluări
- Prevalence of Anemia and Iron Pro File Among Children and Adolescent With Low Socio-Economic StatusDocument5 paginiPrevalence of Anemia and Iron Pro File Among Children and Adolescent With Low Socio-Economic StatusancillaagraynÎncă nu există evaluări
- Ijhoscr 13 220Document9 paginiIjhoscr 13 220ancillaagraynÎncă nu există evaluări
- 08 - 193penggunaan Obat Antiepilepsi Pada KehamilanDocument6 pagini08 - 193penggunaan Obat Antiepilepsi Pada KehamilanErsya MuslihÎncă nu există evaluări
- Fneur 10 00506Document12 paginiFneur 10 00506adityaÎncă nu există evaluări
- Usaid - Physical DR IDDocument66 paginiUsaid - Physical DR IDZi LaÎncă nu există evaluări
- ACE:ARB in ACS PDFDocument9 paginiACE:ARB in ACS PDFancillaagraynÎncă nu există evaluări
- Karakteristik Anafilaksis Pada AnakDocument9 paginiKarakteristik Anafilaksis Pada AnakancillaagraynÎncă nu există evaluări
- Iron Metabolism in Infants and Children: Bo Lönnerdal and Shannon L. KelleherDocument9 paginiIron Metabolism in Infants and Children: Bo Lönnerdal and Shannon L. KelleherancillaagraynÎncă nu există evaluări
- Physical Examination of the Newborn: Classification, Assessment, and Gestational Age DeterminationDocument32 paginiPhysical Examination of the Newborn: Classification, Assessment, and Gestational Age DeterminationancillaagraynÎncă nu există evaluări
- Ijhoscr 13 220Document9 paginiIjhoscr 13 220ancillaagraynÎncă nu există evaluări
- Pulmonary Embolism in Heart FailureDocument1 paginăPulmonary Embolism in Heart FailureancillaagraynÎncă nu există evaluări
- Early, Intensive Statin Treatment Reduces Hard' Cardiovascular Outcomes After Acute Coronary SyndromeDocument3 paginiEarly, Intensive Statin Treatment Reduces Hard' Cardiovascular Outcomes After Acute Coronary SyndromeancillaagraynÎncă nu există evaluări
- Ajr 144 5 879Document16 paginiAjr 144 5 879ancillaagraynÎncă nu există evaluări
- Woman With AcsDocument15 paginiWoman With AcsancillaagraynÎncă nu există evaluări
- The Heart During PregnancyDocument12 paginiThe Heart During PregnancyancillaagraynÎncă nu există evaluări
- CTG HaDocument15 paginiCTG HaNabila SaribanunÎncă nu există evaluări
- Nhs Clinical Evaluation Team Clinical Review Safety Peripheral Intravenous Cannula Report October 2018Document44 paginiNhs Clinical Evaluation Team Clinical Review Safety Peripheral Intravenous Cannula Report October 2018imaguestuserÎncă nu există evaluări
- Mass Production of Bovine Serum AlbuminDocument4 paginiMass Production of Bovine Serum AlbuminInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Local Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankDocument12 paginiLocal Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankJessicaPorterfqmei100% (18)
- Maternal Care Manual: Skills 9Document7 paginiMaternal Care Manual: Skills 9yayitsnayÎncă nu există evaluări
- Clinical ChemistryDocument10 paginiClinical ChemistryChristina AtefÎncă nu există evaluări
- Itrack Advance BrochureDocument2 paginiItrack Advance BrochureHaag-Streit UK (HS-UK)Încă nu există evaluări
- Basic ECG Interpretation Review Questions Flashcards - QuizletDocument5 paginiBasic ECG Interpretation Review Questions Flashcards - Quizletdina sharafÎncă nu există evaluări
- CHARM X Brochure PDFDocument64 paginiCHARM X Brochure PDFSwathi GovindarajanÎncă nu există evaluări
- CLASSIC ARTICLE Clinical Measurement and EvaluationDocument5 paginiCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- Essential Revision Notes For MRCP PDFDocument1.002 paginiEssential Revision Notes For MRCP PDFMontasir Ahmed100% (23)
- Lindsay: VasquezDocument1 paginăLindsay: Vasquezapi-240028260Încă nu există evaluări
- Vaginal Douching: in ReviewDocument7 paginiVaginal Douching: in ReviewNur FadilahÎncă nu există evaluări
- Factors Affecting Severity of Abo-Incompitability Hemolytic Disease of NewbornDocument106 paginiFactors Affecting Severity of Abo-Incompitability Hemolytic Disease of Newbornmahmmoud2228Încă nu există evaluări
- Group 6 Hospitalizing & Simple Past Tense NewDocument36 paginiGroup 6 Hospitalizing & Simple Past Tense NewRahayu TriÎncă nu există evaluări
- Emergency Life Support AlgorithmDocument43 paginiEmergency Life Support AlgorithmDADASDSAÎncă nu există evaluări
- Activity Based ManagementDocument26 paginiActivity Based Managementfortune90100% (2)
- Ecg PDFDocument2 paginiEcg PDFNaveen SharmaÎncă nu există evaluări
- Ano RectalDocument57 paginiAno Rectaldrhemantt1279100% (1)
- GMRS Distal Femur: Global Modular Replacement SystemDocument48 paginiGMRS Distal Femur: Global Modular Replacement SystemSomÎncă nu există evaluări
- Hematopoietic+Stem Cell+TransplantationDocument14 paginiHematopoietic+Stem Cell+TransplantationFabLab EIUÎncă nu există evaluări
- EYE STRUCTURE AND FUNCTIONDocument236 paginiEYE STRUCTURE AND FUNCTIONSherly MydoÎncă nu există evaluări
- Pharmacology Drug ClassificationDocument4 paginiPharmacology Drug ClassificationjetdoctrzÎncă nu există evaluări
- Fluid and Electrolytes BalanceDocument6 paginiFluid and Electrolytes BalanceMichelle Dona MirallesÎncă nu există evaluări
- Agaches Measuring The Skin Non-Invasive Investigations, Physiology, Normal Constants (Philippe Humbert, Ferial Fanian Etc.) (Z-Library)Document1.622 paginiAgaches Measuring The Skin Non-Invasive Investigations, Physiology, Normal Constants (Philippe Humbert, Ferial Fanian Etc.) (Z-Library)irina obrejaÎncă nu există evaluări
- John Beard's 1902 trophoblast cell theory of cancerDocument6 paginiJohn Beard's 1902 trophoblast cell theory of cancerOmar OmarÎncă nu există evaluări
- Drug Education Module PDFDocument73 paginiDrug Education Module PDFChenrose CaliboÎncă nu există evaluări
- Microbiology and Parasitology - Activity 4 The Control of DiseaseDocument3 paginiMicrobiology and Parasitology - Activity 4 The Control of DiseaseClaro M. GarchitorenaÎncă nu există evaluări
- Warfarin LeafletDocument2 paginiWarfarin LeafletchampbeeÎncă nu există evaluări
- Chest Pain ProtocolDocument7 paginiChest Pain Protocolomar kmr97Încă nu există evaluări
- Hypoxia: Hypoxic Injury To CellsDocument5 paginiHypoxia: Hypoxic Injury To CellsUloko ChristopherÎncă nu există evaluări