S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Jri-19-32 (Internasional) PDFDocument7 paginiJri-19-32 (Internasional) PDFIkafitriyaniÎncă nu există evaluări
- 2 - Naskah MarhaeniDocument29 pagini2 - Naskah MarhaeniFarah Nuratna PertiwiÎncă nu există evaluări
- 7001 1 11908 1 10 20131029 PDFDocument10 pagini7001 1 11908 1 10 20131029 PDFIkafitriyaniÎncă nu există evaluări
- CP MastitisDocument11 paginiCP MastitisIkafitriyaniÎncă nu există evaluări
- Surat LamaranDocument1 paginăSurat LamaranIkafitriyaniÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
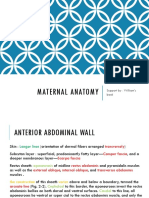
- Chapter 2 Maternal Anatomy WilliamsDocument60 paginiChapter 2 Maternal Anatomy WilliamsDiskaAstariniÎncă nu există evaluări
- Uterine Fibroid EmbolizationDocument2 paginiUterine Fibroid EmbolizationWasim ShaheenÎncă nu există evaluări
- Placenta PreviaDocument19 paginiPlacenta Previarosekatekate929Încă nu există evaluări
- How Do Organisms Reproduce Class 10 Notes Science Chapter 8 - Learn CBSEDocument20 paginiHow Do Organisms Reproduce Class 10 Notes Science Chapter 8 - Learn CBSEPranav MurkumbiÎncă nu există evaluări
- ContractedDocument15 paginiContractedswapnil3250Încă nu există evaluări
- A Study On Artav Vaha Srotas and It's MulsthanaDocument4 paginiA Study On Artav Vaha Srotas and It's MulsthanaEditor IJTSRDÎncă nu există evaluări
- NCM 107maternal FinalsDocument84 paginiNCM 107maternal FinalsFranz goÎncă nu există evaluări
- Ain Shams MCQDocument84 paginiAin Shams MCQمعتز حرارةÎncă nu există evaluări
- Pelvis II (Snell)Document7 paginiPelvis II (Snell)Mich Therese AbejeroÎncă nu există evaluări
- Active Management of Third Stage of LabourDocument27 paginiActive Management of Third Stage of LabourNagamalar RajendraÎncă nu există evaluări
- Abortion: Causes, Types and ManagementDocument39 paginiAbortion: Causes, Types and ManagementEverly Kay Fe ContadorÎncă nu există evaluări
- Combined Science Form 2 Mid Year 2018: Section A (10MARKS)Document3 paginiCombined Science Form 2 Mid Year 2018: Section A (10MARKS)Tafadzwa MunyatiÎncă nu există evaluări
- End of Rotation ExamsDocument104 paginiEnd of Rotation Examsmelkizedeck mbangwaÎncă nu există evaluări
- Notes On Subfertility AssessmentDocument5 paginiNotes On Subfertility AssessmentHassen ZabalaÎncă nu există evaluări
- Reproductive System - Male and FemaleDocument27 paginiReproductive System - Male and FemaleJerome CameroÎncă nu există evaluări
- Obstetrics Study Guide 2: in The Name of GodDocument122 paginiObstetrics Study Guide 2: in The Name of GodGa B B OrlonganÎncă nu există evaluări
- Ong Cases Final-1Document49 paginiOng Cases Final-1Cedric KyekyeÎncă nu există evaluări
- Nclex Obstetrics Practice ExamDocument18 paginiNclex Obstetrics Practice Examchie9268Încă nu există evaluări
- NCM 109 Midterm QuizzesDocument6 paginiNCM 109 Midterm QuizzesclarÎncă nu există evaluări
- Anatomy and Physiology of Female Reproductive SystemDocument5 paginiAnatomy and Physiology of Female Reproductive SystemNURSETOPNOTCHER80% (5)
- DR - PreeclapmsiaDocument104 paginiDR - Preeclapmsiariel100% (14)
- Ob-Gyne: Obstetric History and PEDocument6 paginiOb-Gyne: Obstetric History and PEPorori BookshopÎncă nu există evaluări
- Reproductive System QuizDocument3 paginiReproductive System QuizJONEL FONTILLASÎncă nu există evaluări
- Uterine AbnormalityDocument8 paginiUterine AbnormalityberylianamayaÎncă nu există evaluări
- Baby in The WombDocument19 paginiBaby in The Wombsatish000380% (5)
- Science 5.q2.week1Document5 paginiScience 5.q2.week1Hazy Jade Hombrog RugaÎncă nu există evaluări
- Drug Ang NCPDocument9 paginiDrug Ang NCPMelanie GaledoÎncă nu există evaluări
- Pre Natal CareDocument3 paginiPre Natal CareRoseanne SaraÎncă nu există evaluări
- USMLE Questions SummarizedDocument85 paginiUSMLE Questions SummarizedJamesIwu89% (19)
- NLM Classification: Worldwide Source of Medical Library ClassificationDocument1 paginăNLM Classification: Worldwide Source of Medical Library ClassificationFrancisca CuellarÎncă nu există evaluări