S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
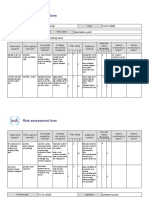
- Risk Assessment Project Iosh - MsDocument2 paginiRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Critical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiDocument5 paginiCritical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiPABLO RAMIRO AGUILAR GONZALEZÎncă nu există evaluări
- Nursing Exam Questions Practice Test VDocument6 paginiNursing Exam Questions Practice Test VTiffany D'Alessandro Gordon94% (18)
- Eric Dollard MWO Update 2012Document21 paginiEric Dollard MWO Update 2012pic2007100% (7)
- Thermal Imaging Tech ResourceDocument20 paginiThermal Imaging Tech Resourceskimav86100% (1)
- Bouncing BallDocument5 paginiBouncing Ballyamamoto1070% (10)
- Congenital Heart Defects Test Five Nursing FourDocument6 paginiCongenital Heart Defects Test Five Nursing FourTiffany D'Alessandro GordonÎncă nu există evaluări
- Statistical Mechanics PDFDocument578 paginiStatistical Mechanics PDFraymon6666100% (6)
- My Ideal Home: Name No. Class Date Mark TeacherDocument5 paginiMy Ideal Home: Name No. Class Date Mark TeacherQuadrado MágicoÎncă nu există evaluări
- Morning in Nagrebcan - Manuel E. ArguillaDocument8 paginiMorning in Nagrebcan - Manuel E. ArguillaClara Buenconsejo75% (16)
- 8/24/2010 Lecture Condensed To 3 PagesDocument3 pagini8/24/2010 Lecture Condensed To 3 PagesTiffany D'Alessandro GordonÎncă nu există evaluări
- Bariatric DrugsDocument3 paginiBariatric DrugsTiffany D'Alessandro Gordon100% (1)
- Everything I Have Highlighted From 8/24/10 LecturesDocument1 paginăEverything I Have Highlighted From 8/24/10 LecturesTiffany D'Alessandro GordonÎncă nu există evaluări
- Nursing Exam Test V Crisis InterventionDocument3 paginiNursing Exam Test V Crisis InterventionTiffany D'Alessandro GordonÎncă nu există evaluări
- Valvula Reguladoras Pilotados DANFOSSDocument2 paginiValvula Reguladoras Pilotados DANFOSSJurandir Laureano SILVA JUNIORÎncă nu există evaluări
- Hirschsprung's Disease - AthigamanDocument128 paginiHirschsprung's Disease - Athigamanprived100% (4)
- E2870-13 Standard Test Method For Evaluating RelativDocument6 paginiE2870-13 Standard Test Method For Evaluating RelativA MusaverÎncă nu există evaluări
- Board of Technical Education Uttar Pradesh Lucknow: CODE 2298Document2 paginiBoard of Technical Education Uttar Pradesh Lucknow: CODE 2298Md Shaaz100% (1)
- Feu Sharing Stress MNGTDocument58 paginiFeu Sharing Stress MNGTsquidsexoÎncă nu există evaluări
- Apti 2Document17 paginiApti 2Arunkumar MurugappanÎncă nu există evaluări
- Version 2 Dog Legged Stair ES EN 1992-1-1 2015Document29 paginiVersion 2 Dog Legged Stair ES EN 1992-1-1 2015Khaja100% (2)
- Portable Load Banks: CressallDocument1 paginăPortable Load Banks: CressallYashveer26Încă nu există evaluări
- Starlift MetricDocument2 paginiStarlift MetricCralesÎncă nu există evaluări
- CF1900SS-DF Example Spec - Rev1Document1 paginăCF1900SS-DF Example Spec - Rev1parsiti unnesÎncă nu există evaluări
- Geo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDocument5 paginiGeo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDevendrasinh PadhiyarÎncă nu există evaluări
- GenesDocument33 paginiGenesJerick RoxasÎncă nu există evaluări
- RT Offer L-Seam-14.01.2023Document1 paginăRT Offer L-Seam-14.01.2023Eswar Enterprises QcÎncă nu există evaluări
- Revision For The First 1 English 8Document6 paginiRevision For The First 1 English 8hiidaxneee urrrmÎncă nu există evaluări
- NEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andDocument90 paginiNEET MADE EJEE Complete Handwritten Formulae Chemistry NEET andliyanderÎncă nu există evaluări
- Water Treatment Lecture 4Document34 paginiWater Treatment Lecture 4pramudita nadiahÎncă nu există evaluări
- Essenza Refurbished Siemens MRI MachineDocument2 paginiEssenza Refurbished Siemens MRI Machinetech.arnicahealthÎncă nu există evaluări
- Transformation of Modern Library in To Green Library For Sustaining FutureDocument7 paginiTransformation of Modern Library in To Green Library For Sustaining FutureHardik AnandÎncă nu există evaluări
- Prince Hydraulics Wolverine Adjustable Flow Control Valve Offered by PRC Industrial SupplyDocument1 paginăPrince Hydraulics Wolverine Adjustable Flow Control Valve Offered by PRC Industrial SupplyPRC Industrial SupplyÎncă nu există evaluări
- Devi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswariDocument7 paginiDevi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswaribrindaÎncă nu există evaluări
- CCNP 300 410 ENARSI NetworkTUT 26 5 2021Document104 paginiCCNP 300 410 ENARSI NetworkTUT 26 5 2021Olga BradyÎncă nu există evaluări
- IBH Link UA Manual PDFDocument302 paginiIBH Link UA Manual PDFjavixl1Încă nu există evaluări