S-ar putea să vă placă și
- Assessment Summary / Cover Sheet: Student Assessment CHCCCS015 Provide Individualised SupportDocument16 paginiAssessment Summary / Cover Sheet: Student Assessment CHCCCS015 Provide Individualised SupportGurpreet Singh Wirring67% (3)
- CHCCCS023 Support Independence and WellbeingDocument22 paginiCHCCCS023 Support Independence and WellbeingSushma karkiÎncă nu există evaluări
- Assessment Guide: CHCDIS007 Facilitate The Empowerment of People With A DisabilityDocument23 paginiAssessment Guide: CHCDIS007 Facilitate The Empowerment of People With A DisabilitySamir Bhandari100% (1)
- CHCAGE002Document16 paginiCHCAGE002Niraj NepalÎncă nu există evaluări
- CHCHCS001 Home & Community SupportDocument23 paginiCHCHCS001 Home & Community SupportSibani KarÎncă nu există evaluări
- Classroom Activity CHCDIS003Document4 paginiClassroom Activity CHCDIS003Sonam GurungÎncă nu există evaluări
- SAB CHCAGE005 Provide Support To People Living With DementiaDocument114 paginiSAB CHCAGE005 Provide Support To People Living With DementiaAnonymous wWCGc6fzUX100% (3)
- Empowerment of Older PersonDocument9 paginiEmpowerment of Older PersonSoniya Ghising100% (2)
- CHCCCS011 Meet Personal Support Needs SAB v3.1 THEORYDocument28 paginiCHCCCS011 Meet Personal Support Needs SAB v3.1 THEORYAbhishek Dhungel50% (6)
- BSBWHS302Document17 paginiBSBWHS302Akis Drallos0% (3)
- Task 1 Meet Personal NeedsDocument6 paginiTask 1 Meet Personal Needsdev kumar67% (3)
- TMG Assessment Cover Sheet & Learner Assessment PackDocument35 paginiTMG Assessment Cover Sheet & Learner Assessment PackMD NASIR UDDIN33% (3)
- CHCPAL001 Student Assessment Booklet - AGE (ID 98478)Document49 paginiCHCPAL001 Student Assessment Booklet - AGE (ID 98478)Francis Dave Peralta Bitong50% (2)
- CHCPAL001 Deliver Care Services Using A Palliative ApproachDocument122 paginiCHCPAL001 Deliver Care Services Using A Palliative Approachdev kumar75% (4)
- Chcage001 GaganDocument6 paginiChcage001 GaganNimesh Parmar67% (3)
- Classroom Activity CHCDIS007Document3 paginiClassroom Activity CHCDIS007Sonam Gurung100% (1)
- CHCCCS015 Provide Individualised Support SAB v3.2 THEORYDocument27 paginiCHCCCS015 Provide Individualised Support SAB v3.2 THEORYShufali Sherchan100% (1)
- CHCDIS005 Develop and Provide Person Centred Service Responses CompleteDocument22 paginiCHCDIS005 Develop and Provide Person Centred Service Responses Completepriyashvi k100% (2)
- Showdoc CFMDocument97 paginiShowdoc CFMH.D50% (2)
- HLTHPS007 STDNT Assess BK V3 29.05.19Document139 paginiHLTHPS007 STDNT Assess BK V3 29.05.19Bùi Thắng50% (2)
- Task 2 Meet Personal NeedsDocument3 paginiTask 2 Meet Personal Needsdev kumarÎncă nu există evaluări
- Assessment # 5Document33 paginiAssessment # 5Gurpreet Singh Wirring50% (2)
- Home and Community Support CHCHCS001 Provide Home and Community Support ServicesDocument31 paginiHome and Community Support CHCHCS001 Provide Home and Community Support Serviceskul1990100% (1)
- Assignment CHCHCS001 Provide Home and Community Support ServicesDocument2 paginiAssignment CHCHCS001 Provide Home and Community Support Serviceskul199067% (6)
- Shyna Assessment 2Document17 paginiShyna Assessment 2dev kumar100% (1)
- CHCAGE003.02.2 Case Studies v2.1 006Document42 paginiCHCAGE003.02.2 Case Studies v2.1 006rana ikram0% (1)
- CHCLEG001 Assessment - Tahlia O'Keefe-QuinnDocument3 paginiCHCLEG001 Assessment - Tahlia O'Keefe-QuinnSamantha Abel100% (4)
- CHCDIS007 Facilitate The Empowerment of People With Disability6Document14 paginiCHCDIS007 Facilitate The Empowerment of People With Disability6yESHEy TÎncă nu există evaluări
- E1144 Module2 Assessment3 SAQrubric 32469 03 v2 3 THyde 1 01 04 2020 2159Document25 paginiE1144 Module2 Assessment3 SAQrubric 32469 03 v2 3 THyde 1 01 04 2020 2159tetyana0% (1)
- CHCAGE002 Implement Falls Prevention SAB v3.1 THEORYDocument20 paginiCHCAGE002 Implement Falls Prevention SAB v3.1 THEORYAbhishek Dhungel33% (3)
- Guidelines For Infection Prevention and Control - IrlandaDocument120 paginiGuidelines For Infection Prevention and Control - IrlandaRaquel LopesÎncă nu există evaluări
- CHCPAL001 Student Assessment Booklet - AGE (ID 98478)Document52 paginiCHCPAL001 Student Assessment Booklet - AGE (ID 98478)Show Ssti20% (5)
- Learner Guide CHCCCS023 Support Independence and Well Being: International CollegeDocument172 paginiLearner Guide CHCCCS023 Support Independence and Well Being: International CollegeElsie GibbsÎncă nu există evaluări
- Individual Support Work Skills Workshop Student Assessments BookletDocument68 paginiIndividual Support Work Skills Workshop Student Assessments BookletPranav Prajapati0% (2)
- HLTWHS002 PDFDocument4 paginiHLTWHS002 PDFJase Harrison25% (4)
- HLTINF006 Assessment Task 1 With AnswerDocument8 paginiHLTINF006 Assessment Task 1 With AnswerRebeca Raducu100% (1)
- CHCLEG003 - Assignment 1 Task 1 - Case ScenarioDocument3 paginiCHCLEG003 - Assignment 1 Task 1 - Case ScenarioBrigham Hunt100% (3)
- HLTWHS002 Follow Safe Practices For Direct Client Care SAB v3.0 - THEORYDocument22 paginiHLTWHS002 Follow Safe Practices For Direct Client Care SAB v3.0 - THEORYSujan Adhikari100% (2)
- CHCCOM005 Communication and Work in Health and Community Services 4Document13 paginiCHCCOM005 Communication and Work in Health and Community Services 4yESHEy TÎncă nu există evaluări
- CHCPA301B Deliver Care Services Using A Palliative ApproachDocument73 paginiCHCPA301B Deliver Care Services Using A Palliative ApproachBhakta Chand ThakuriÎncă nu există evaluări
- Chcdis003 Case StudyDocument15 paginiChcdis003 Case StudyRajina MaharjanÎncă nu există evaluări
- Information Book CHC33015 Cert III Individual Support Ageing HACC 2019 v1Document15 paginiInformation Book CHC33015 Cert III Individual Support Ageing HACC 2019 v1Andrew100% (1)
- CHCAGE005 Provide Support To People Living With Dementia SAB v3.2 THEORYDocument34 paginiCHCAGE005 Provide Support To People Living With Dementia SAB v3.2 THEORYAbhishek Dhungel0% (1)
- Chcccs015 Student Workbook Prabina (Word) (c3) .v1.1Document41 paginiChcccs015 Student Workbook Prabina (Word) (c3) .v1.1yESHEy T100% (2)
- Facilitate Individual ServiceDocument15 paginiFacilitate Individual Servicedev kumar100% (2)
- Hltin301c v2 Comply With Infection Control Policies and Procedures in Health WorkDocument76 paginiHltin301c v2 Comply With Infection Control Policies and Procedures in Health Workapi-879674940% (1)
- CHCAGE005 Assessment FINALDocument22 paginiCHCAGE005 Assessment FINALGurpreet Singh Wirring67% (3)
- IS01Document8 paginiIS01Anonymous lSPAn1V100% (1)
- Student Assessment Booklet: CHC33015 C III I SDocument23 paginiStudent Assessment Booklet: CHC33015 C III I SSibani Kar0% (1)
- CHCCCS011 Meet Personal Support Needs Resource InterCare1Document146 paginiCHCCCS011 Meet Personal Support Needs Resource InterCare1komalbajaj100% (1)
- Cert III Individual Support - SAI Education InstituteDocument6 paginiCert III Individual Support - SAI Education InstituteNickÎncă nu există evaluări
- Assessment 011 1Document12 paginiAssessment 011 1ManawÎncă nu există evaluări
- Topic 1: Before You Begin Determine Personal Support RequirementsDocument20 paginiTopic 1: Before You Begin Determine Personal Support Requirementsdefa reyÎncă nu există evaluări
- Task 3 CHCCOM005Document8 paginiTask 3 CHCCOM005Angela BravoÎncă nu există evaluări
- Task 2 CHCCOM005Document9 paginiTask 2 CHCCOM005Angela Bravo100% (2)
- Follow Safe Practices For Direct Client Care - DoneDocument55 paginiFollow Safe Practices For Direct Client Care - DoneSebin George0% (7)
- HLTINF001 Learner Guide V1 June 20Document94 paginiHLTINF001 Learner Guide V1 June 20Kabita123 NepzzÎncă nu există evaluări
- Assessment Summary / Cover Sheet: Click or Tap Here To Enter Text. Click or Tap Here To Enter TextDocument15 paginiAssessment Summary / Cover Sheet: Click or Tap Here To Enter Text. Click or Tap Here To Enter TextGurpreet Singh WirringÎncă nu există evaluări
- Food Counselling. How To Motivate People To Change Eating HabitsDe la EverandFood Counselling. How To Motivate People To Change Eating HabitsÎncă nu există evaluări
- Caring for the Carers: A Guide to Help Paid Carers for People with Learning DisabilitiesDe la EverandCaring for the Carers: A Guide to Help Paid Carers for People with Learning DisabilitiesÎncă nu există evaluări
- Articulo TapentadolDocument5 paginiArticulo TapentadolSol SalazarÎncă nu există evaluări
- RCDSO Guidelines Role of OpioidsDocument16 paginiRCDSO Guidelines Role of OpioidsMonaÎncă nu există evaluări
- BIO MAT TESTIMONIALS - Doc0001Document30 paginiBIO MAT TESTIMONIALS - Doc0001Nicole WeatherleyÎncă nu există evaluări
- MedicamenteDocument3 paginiMedicamentecraciun monicaÎncă nu există evaluări
- Chemistry of Opioid Analgesics PHA 4220 - Neurology PharmacotherapeuticsDocument13 paginiChemistry of Opioid Analgesics PHA 4220 - Neurology PharmacotherapeuticsethanalbertÎncă nu există evaluări
- 2017.6.28 DR - Klein Response To Proposed Removal WExhibits ReducedDocument416 pagini2017.6.28 DR - Klein Response To Proposed Removal WExhibits ReducedmikekvolpeÎncă nu există evaluări
- UNIT 1: Nursing Interventions To Promote Healthy Physiologic Responses: Comfort and PainDocument14 paginiUNIT 1: Nursing Interventions To Promote Healthy Physiologic Responses: Comfort and Painlouie tibarÎncă nu există evaluări
- Narcotic Drugs: Opium Herion Codeine Tramadol MorphineDocument9 paginiNarcotic Drugs: Opium Herion Codeine Tramadol MorphineSyed renobaÎncă nu există evaluări
- NURSING CARE PLAN The Child Undergoing Surgery For ScoliosisDocument3 paginiNURSING CARE PLAN The Child Undergoing Surgery For ScoliosisscrewdriverÎncă nu există evaluări
- Pain Monitoring ChartDocument2 paginiPain Monitoring ChartAmith VijayanÎncă nu există evaluări
- Hasil Uji Disolusi PCT 500 MG Kel 6Document7 paginiHasil Uji Disolusi PCT 500 MG Kel 6ayangaudia3316Încă nu există evaluări
- Manual - HALODocument42 paginiManual - HALOsanthigiÎncă nu există evaluări
- How To Use The Opioid Conversion GuideDocument17 paginiHow To Use The Opioid Conversion Guidemun_chloeÎncă nu există evaluări
- A Cochrane Review of Superficial Heat or ColdDocument9 paginiA Cochrane Review of Superficial Heat or ColdIvanFierroÎncă nu există evaluări
- Referat Analgesik OpioidDocument25 paginiReferat Analgesik OpioidDeny Prima OÎncă nu există evaluări
- Epidural Analgesia in Labour Management and CareDocument29 paginiEpidural Analgesia in Labour Management and CareMihai IoanÎncă nu există evaluări
- Aling Juana, 42 Years Old, FemaleDocument2 paginiAling Juana, 42 Years Old, FemaleGenynne RagasaÎncă nu există evaluări
- Pain AssessentDocument9 paginiPain AssessentJoanna RachelÎncă nu există evaluări
- Task Force RecommendationsDocument3 paginiTask Force RecommendationsDan LehrÎncă nu există evaluări
- 812-Article Text-2928-1-10-20191129 (PMR)Document6 pagini812-Article Text-2928-1-10-20191129 (PMR)Azza SintaÎncă nu există evaluări
- Guinea Pigs PDFDocument1 paginăGuinea Pigs PDFYaserAbbasiÎncă nu există evaluări
- WongLitWan PDFDocument507 paginiWongLitWan PDFdannyÎncă nu există evaluări
- Obese ParturientDocument7 paginiObese Parturientbilly wilsonÎncă nu există evaluări
- Cervicogenic HeadacheDocument7 paginiCervicogenic Headachemeta456Încă nu există evaluări
- Assessing Pain in Patients: Art ScienceDocument5 paginiAssessing Pain in Patients: Art ScienceShweta SheoranÎncă nu există evaluări
- E.G. 1) Pain Management PDFDocument4 paginiE.G. 1) Pain Management PDFfocus16hoursgmailcomÎncă nu există evaluări
- Algology ModuleDocument2 paginiAlgology ModulerosanowardÎncă nu există evaluări
- Nri2022 8336561Document14 paginiNri2022 8336561Carolina SidabutarÎncă nu există evaluări
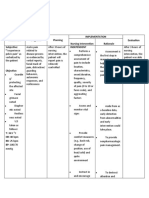
- Pelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentDocument2 paginiPelagio, Shiena Mae B. BSN Ii-A CASE: Cervical Cancer Implementation Nursing Intervention Rationale Evaluation Subjective: "I Experience IndependentShiena Mae PelagioÎncă nu există evaluări
- Nursing Report MateriDocument2 paginiNursing Report MaterifitriÎncă nu există evaluări