S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- 2 - WIG ORATION - Sept 16 2018 - Murthy - AbstractDocument2 pagini2 - WIG ORATION - Sept 16 2018 - Murthy - AbstractAmitranjan BasuÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Arindam Chakrabarty (2011) Troubles With A Second Self The Problem of Other Minds in 11th Century Indian and 20th Century Western Philosophy PDFDocument13 paginiArindam Chakrabarty (2011) Troubles With A Second Self The Problem of Other Minds in 11th Century Indian and 20th Century Western Philosophy PDFAmitranjan BasuÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Epidemics and Pandemics in India Throughout History A Review Article, 2019 PDFDocument8 paginiEpidemics and Pandemics in India Throughout History A Review Article, 2019 PDFAmitranjan BasuÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- A. W. Woodruff (1957) Medical Training and Research in India To-DayDocument4 paginiA. W. Woodruff (1957) Medical Training and Research in India To-DayAmitranjan BasuÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Abbe Faria (2014) A Compendium of Articles and Photographs PDFDocument275 paginiAbbe Faria (2014) A Compendium of Articles and Photographs PDFAmitranjan Basu100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- 2 - WIG ORATION - Sept 16 2018 - Murthy - AbstractDocument2 pagini2 - WIG ORATION - Sept 16 2018 - Murthy - AbstractAmitranjan BasuÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- An African's Mental Outlook in Britain, BMJ, 1958 PDFDocument3 paginiAn African's Mental Outlook in Britain, BMJ, 1958 PDFAmitranjan BasuÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Therapy Wars Contention and Convergence in Differing Clinical Approaches, 1990Document425 paginiTherapy Wars Contention and Convergence in Differing Clinical Approaches, 1990Amitranjan Basu100% (2)
- Colonel Sykes (1860) Traits of Indian CharacterDocument30 paginiColonel Sykes (1860) Traits of Indian CharacterAmitranjan BasuÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Padmasrı's Nagarasarvasva and The World of Medieval Kamasastra, 2011Document22 paginiPadmasrı's Nagarasarvasva and The World of Medieval Kamasastra, 2011Amitranjan Basu100% (1)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Auroville and The Paradox of A Postcolonial Utopia, 2012Document31 paginiAuroville and The Paradox of A Postcolonial Utopia, 2012Amitranjan BasuÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Book Review of 'Nishir Dak' by Asim ChatterjeeDocument3 paginiBook Review of 'Nishir Dak' by Asim ChatterjeeAmitranjan BasuÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Benoy Ghose (1960) The Colonial Beginnings of Calcutta Urbanisation Without IndustrialisationDocument6 paginiBenoy Ghose (1960) The Colonial Beginnings of Calcutta Urbanisation Without IndustrialisationAmitranjan BasuÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Bengali Stage 1795-1873 by Brajendranath Banerjee, 1948Document70 paginiBengali Stage 1795-1873 by Brajendranath Banerjee, 1948Amitranjan BasuÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- DefianceDocument582 paginiDefianceCarl Kerri JohnsonÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Rati Viparite' Gitagovinda and Erotic (Trans) Migrations in Nineteenth Century Bengal I, 2012Document12 paginiRati Viparite' Gitagovinda and Erotic (Trans) Migrations in Nineteenth Century Bengal I, 2012Amitranjan BasuÎncă nu există evaluări
- On The Gipsies of Bengal - Rajendralal Mitra, 1867Document4 paginiOn The Gipsies of Bengal - Rajendralal Mitra, 1867Amitranjan BasuÎncă nu există evaluări
- British Medicine in India, 1907Document10 paginiBritish Medicine in India, 1907Amitranjan BasuÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- 'Mishtanna-Pak', 2nd Ed, 1904. A Book On Bengali Sweet Making by Bipradas MukhopadhyayDocument9 pagini'Mishtanna-Pak', 2nd Ed, 1904. A Book On Bengali Sweet Making by Bipradas MukhopadhyayAmitranjan BasuÎncă nu există evaluări
- Mishtanna-Pak', 2nd Ed, 1904. A Book On Bengali Sweet Making by Bipradas MukhopadhyayDocument72 paginiMishtanna-Pak', 2nd Ed, 1904. A Book On Bengali Sweet Making by Bipradas MukhopadhyayAmitranjan BasuÎncă nu există evaluări
- Kalikata Kamalalaya, 1823Document56 paginiKalikata Kamalalaya, 1823Amitranjan Basu0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Mishtanna-Pak, 2nd Ed, 1904 by Bipradas MukhopadhyayDocument5 paginiMishtanna-Pak, 2nd Ed, 1904 by Bipradas MukhopadhyayAmitranjan BasuÎncă nu există evaluări
- 'Mishtanna-Pak', 2nd Ed, 1904 - A Book On Bengali Sweet MakingDocument10 pagini'Mishtanna-Pak', 2nd Ed, 1904 - A Book On Bengali Sweet MakingAmitranjan BasuÎncă nu există evaluări
- Approaches To HistoryDocument90 paginiApproaches To Historysanazh100% (2)
- Humanistic PsychotherapyDocument26 paginiHumanistic PsychotherapyAmitranjan BasuÎncă nu există evaluări
- Ashis Nandy-The Ambivalence About Gandhi in Himal 2006Document4 paginiAshis Nandy-The Ambivalence About Gandhi in Himal 2006Amitranjan BasuÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Hundred Years of Manto KafilaDocument18 paginiA Hundred Years of Manto KafilaAmitranjan BasuÎncă nu există evaluări
- Ashis Nandy NM Lecture TranscriptDocument10 paginiAshis Nandy NM Lecture Transcriptphronesis76Încă nu există evaluări
- COVID-19 Vaccination PlanDocument46 paginiCOVID-19 Vaccination PlanFOX 17 NewsÎncă nu există evaluări
- Literature Review of Swine FluDocument5 paginiLiterature Review of Swine Fluc5qd4nn8100% (1)
- Book Review: Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 2nd Ed. by W. Richard Webb and Charles R. HigginsDocument1 paginăBook Review: Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 2nd Ed. by W. Richard Webb and Charles R. HigginsDr Apoorva ReddyÎncă nu există evaluări
- NEWS RELEASE Leonard Horowitz AffidavitDocument40 paginiNEWS RELEASE Leonard Horowitz AffidavitJean-Paul de Montréal100% (2)
- Flu UpdateDocument36 paginiFlu UpdateDan ShepardÎncă nu există evaluări
- Emerging and Re-Emerging DiseasesDocument27 paginiEmerging and Re-Emerging Diseasesلؤي فارس100% (1)
- Nelson Central School: Term 3Document4 paginiNelson Central School: Term 3staffncs100% (2)
- Covid-19 and Its Global Impacts: Essay For Css/Pms (2880 WORDS)Document28 paginiCovid-19 and Its Global Impacts: Essay For Css/Pms (2880 WORDS)Agha Khan DurraniÎncă nu există evaluări
- Retraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument1 paginăRetraction-Ileal-lymphoid-nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenOutlawHealthÎncă nu există evaluări
- MAPEH 8 Quarter 3 WEEK 5-6 (MODULE) MusicDocument4 paginiMAPEH 8 Quarter 3 WEEK 5-6 (MODULE) MusicMirela CalubayanÎncă nu există evaluări
- 10.30.2009 Haslett High SchoolDocument15 pagini10.30.2009 Haslett High SchoolhaslettstudentmediaÎncă nu există evaluări
- Emerging Zoonoses: I. W. FongDocument255 paginiEmerging Zoonoses: I. W. FongfdfdfdfÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Viswanath POTC 1632764Document328 paginiViswanath POTC 1632764Ana Cristina Felício Rios MirandaÎncă nu există evaluări
- H1N1 Swine FlupptDocument28 paginiH1N1 Swine FlupptDr. Hesham Zaatar100% (1)
- Dynamic Models of Infectious DiseaseDocument269 paginiDynamic Models of Infectious DiseaseFabianno Ferreira DutraÎncă nu există evaluări
- FA - Booklet idsMED Fair - V5Document134 paginiFA - Booklet idsMED Fair - V5Reza Yuni SandraÎncă nu există evaluări
- Syllabus Ar101 Spring 2012-1Document5 paginiSyllabus Ar101 Spring 2012-1lmonsterzÎncă nu există evaluări
- Assignment 3: Stella ModelDocument9 paginiAssignment 3: Stella Modeld066915Încă nu există evaluări
- The Value of Nothing - Slow PoliticsDocument6 paginiThe Value of Nothing - Slow PoliticsRaj PatelÎncă nu există evaluări
- The Autobiography of The Other Lady GagaDocument7 paginiThe Autobiography of The Other Lady GagaElenear De OcampoÎncă nu există evaluări
- St. Clair County Pandemic Influenza PlanDocument143 paginiSt. Clair County Pandemic Influenza PlanErin Richey KSDKÎncă nu există evaluări
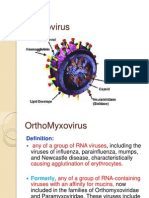
- OrthomyxovirusesDocument39 paginiOrthomyxovirusesማላያላም ማላያላምÎncă nu există evaluări
- Inside Track - October 2009Document4 paginiInside Track - October 2009Falls Church City Public SchoolsÎncă nu există evaluări
- Reading Articles SET - DDocument22 paginiReading Articles SET - DRiddhima MahajanÎncă nu există evaluări
- The Bird Flu and YouDocument15 paginiThe Bird Flu and YouMahogony ScottÎncă nu există evaluări
- Avian Influenza H5N1 VirusDocument27 paginiAvian Influenza H5N1 VirusHarsh Purwar100% (3)
- DLP HEALTH8 APRIL17 2023 Emerging and Re Emerging DiseasesDocument6 paginiDLP HEALTH8 APRIL17 2023 Emerging and Re Emerging DiseasesAljun MansalapusÎncă nu există evaluări
- A h1n1 PathophysiologyDocument11 paginiA h1n1 PathophysiologyJayson RNÎncă nu există evaluări
- CoViD 19 Vaccines A Population Marked ToDocument8 paginiCoViD 19 Vaccines A Population Marked TorentacuraÎncă nu există evaluări
- Unusual Purchasing Behavior During The Early Stages of The COVID19 Pandemic... The Stimulus-Organism-Response ApproachDocument13 paginiUnusual Purchasing Behavior During The Early Stages of The COVID19 Pandemic... The Stimulus-Organism-Response ApproachRishab ManochaÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări