S-ar putea să vă placă și
- Acute Surgical Topics: An Infographic GuideDe la EverandAcute Surgical Topics: An Infographic GuideÎncă nu există evaluări
- Ambrisentan: Jamie D. Croxtall and Susan J. KeamDocument10 paginiAmbrisentan: Jamie D. Croxtall and Susan J. KeamElden Kyle BillonesÎncă nu există evaluări
- Drug Prescribing For Dentistry: Analgesic and Antibiotic Contraindications and Cautions Supplement May 2021Document9 paginiDrug Prescribing For Dentistry: Analgesic and Antibiotic Contraindications and Cautions Supplement May 2021ABÎncă nu există evaluări
- AACE Postmenopausal Osteoporosis Treatment Algorithm Update 022020Document1 paginăAACE Postmenopausal Osteoporosis Treatment Algorithm Update 022020Abby AramintaÎncă nu există evaluări
- Client Profile Log Antenatal - CompleteDocument5 paginiClient Profile Log Antenatal - CompleteLinea GreeneÎncă nu există evaluări
- Guidelines DVT PrimaryDocument2 paginiGuidelines DVT PrimaryRAMARÎncă nu există evaluări
- Tamoxifen NolvadexDocument1 paginăTamoxifen NolvadexAdrianne Bazo100% (1)
- Drug Study 2Document2 paginiDrug Study 2HeavenÎncă nu există evaluări
- LHF Asthma Algorithm2021Document1 paginăLHF Asthma Algorithm2021FatimaÎncă nu există evaluări
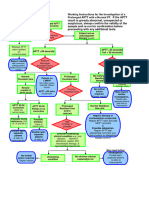
- Working Instructions Investigation of Prolonged APTTDocument1 paginăWorking Instructions Investigation of Prolonged APTTtadeariba1Încă nu există evaluări
- NEL/NCL BRVO Pathway: (Box A) Anti-VEGF (Box B) SteroidDocument1 paginăNEL/NCL BRVO Pathway: (Box A) Anti-VEGF (Box B) SteroidElika Dwi CahyaniÎncă nu există evaluări
- SDCEP Anticoagulants Quick Reference GuideDocument4 paginiSDCEP Anticoagulants Quick Reference Guidejpatel24Încă nu există evaluări
- 3 Minute Exam DFSDocument2 pagini3 Minute Exam DFSWeeChuan NgÎncă nu există evaluări
- Dental MedicineDocument59 paginiDental Medicinechh56k6tndÎncă nu există evaluări
- Anticoagulant Oral GuidelinesforprescribingmonitoringandmanagementDocument29 paginiAnticoagulant Oral GuidelinesforprescribingmonitoringandmanagementJamie PalmeriÎncă nu există evaluări
- Doacs For VteDocument10 paginiDoacs For VteAhmed MohammedÎncă nu există evaluări
- Direct Oral Anticoagulants (DOACs) For Treatment of DVTDocument11 paginiDirect Oral Anticoagulants (DOACs) For Treatment of DVTLuana MÎncă nu există evaluări
- Low Molecular Weight Heparins Summary Prescribing Guide Version 1.3Document14 paginiLow Molecular Weight Heparins Summary Prescribing Guide Version 1.3sharief145Încă nu există evaluări
- Ambrisentan: James E. FramptonDocument12 paginiAmbrisentan: James E. FramptonElden Kyle BillonesÎncă nu există evaluări
- Leptospirosis Pathway JULY 2018FINALDocument5 paginiLeptospirosis Pathway JULY 2018FINALNehemiah FranciscoÎncă nu există evaluări
- University of Cebu-Banilad College of NursingDocument4 paginiUniversity of Cebu-Banilad College of NursingMauriceÎncă nu există evaluări
- Pre Anaesthetic Check-UpDocument4 paginiPre Anaesthetic Check-UpUdoy PaulÎncă nu există evaluări
- How To Use The FYI FlagsDocument5 paginiHow To Use The FYI FlagsFuji guruÎncă nu există evaluări
- ICU One Pagers Vent WeaningDocument1 paginăICU One Pagers Vent WeaningHossameldin GamalÎncă nu există evaluări
- ACO Av Med Form 1 V1 02 New 2Document2 paginiACO Av Med Form 1 V1 02 New 2n77t9hvtmgÎncă nu există evaluări
- DSDSSDDocument10 paginiDSDSSDkrischaniÎncă nu există evaluări
- Escalation Guide For Gram-Negative Bacteremia StanfordDocument3 paginiEscalation Guide For Gram-Negative Bacteremia StanfordLuis MedinaÎncă nu există evaluări
- ACO AV Med Form 1 (Paper) - v1.02 - Jul 15 PDFDocument2 paginiACO AV Med Form 1 (Paper) - v1.02 - Jul 15 PDFKen BogleÎncă nu există evaluări
- Canadian Agency (1) - CDR - Complete - Pradax - June-27-11Document5 paginiCanadian Agency (1) - CDR - Complete - Pradax - June-27-11Marcelo UGÎncă nu există evaluări
- PPI DeprescribingDocument1 paginăPPI Deprescribinghairos.izhaÎncă nu există evaluări
- Fill-InDocument2 paginiFill-InALIZA BAKILÎncă nu există evaluări
- NCD Guidelines 2012Document12 paginiNCD Guidelines 2012Nari BurathiÎncă nu există evaluări
- Low Molecular Weigh Heparins Summary Prescribing Guide Version 14Document15 paginiLow Molecular Weigh Heparins Summary Prescribing Guide Version 14alexandr zinchenkoÎncă nu există evaluări
- Form AvmedDocument2 paginiForm Avmedn77t9hvtmgÎncă nu există evaluări
- AACE ACE 2016 Postmenopausal Osteoporosis Treatment Algorithm PDFDocument1 paginăAACE ACE 2016 Postmenopausal Osteoporosis Treatment Algorithm PDFTabs NuñezÎncă nu există evaluări
- Drug StudyDocument10 paginiDrug StudyJONISA THERESE MAE LALANTACONÎncă nu există evaluări
- Pharmacology Concise Notes NEET-PGDocument30 paginiPharmacology Concise Notes NEET-PGMohamed TayyabÎncă nu există evaluări
- Care Plan:, Wrong, Wrong, Wrong, WrongDocument8 paginiCare Plan:, Wrong, Wrong, Wrong, Wronglovelylife theÎncă nu există evaluări
- Medical TherapyDocument6 paginiMedical Therapyvinay reddyÎncă nu există evaluări
- Drug Study - AlfuzosinDocument1 paginăDrug Study - AlfuzosinKian HerreraÎncă nu există evaluări
- Giop Guideline Summary 2022Document7 paginiGiop Guideline Summary 2022adri20121989Încă nu există evaluări
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDocument2 paginiAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasÎncă nu există evaluări
- Drug Study23Document2 paginiDrug Study23Joh Acedo BantingÎncă nu există evaluări
- Drug Study Kathleen Claire ColinioDocument11 paginiDrug Study Kathleen Claire ColinioKathleen ColinioÎncă nu există evaluări
- NIV Algorithm Final Version Jan 2020Document3 paginiNIV Algorithm Final Version Jan 2020AmalÎncă nu există evaluări
- Laminectomy: Notes On PROSPECT RecommendationsDocument5 paginiLaminectomy: Notes On PROSPECT RecommendationsWidya AriatyÎncă nu există evaluări
- CCO IBD Key Issues Downloadable 4Document22 paginiCCO IBD Key Issues Downloadable 4160835Încă nu există evaluări
- Azithromycin Medication PDFDocument1 paginăAzithromycin Medication PDFmp1757Încă nu există evaluări
- Gentamicin SulfateDocument2 paginiGentamicin SulfateVlienkCruzÎncă nu există evaluări
- Drug StudyDocument4 paginiDrug StudyColanag, Ian JohnÎncă nu există evaluări
- 374 FullDocument17 pagini374 FullValentina MerolaÎncă nu există evaluări
- Case Study No. 1 NCP Fdar Drug Study CompilationDocument8 paginiCase Study No. 1 NCP Fdar Drug Study CompilationRosemarie R. ReyesÎncă nu există evaluări
- Case Study No. 1 NCP Fdar Drug Study CompilationDocument8 paginiCase Study No. 1 NCP Fdar Drug Study CompilationRosemarie R. ReyesÎncă nu există evaluări
- Vets Now Surgical Safety ChecklistDocument1 paginăVets Now Surgical Safety ChecklistVeterinarios de ArgentinaÎncă nu există evaluări
- Handbook of Surgical Care For House OfficersDocument20 paginiHandbook of Surgical Care For House OfficersCharity AtsuÎncă nu există evaluări
- Chiron Et Al 2011 EpilepsiaDocument4 paginiChiron Et Al 2011 EpilepsiaAlexandra PrikopÎncă nu există evaluări
- Clinical Guideline Suspected Adrenal IncidentalomaDocument3 paginiClinical Guideline Suspected Adrenal IncidentalomaMica SaeronÎncă nu există evaluări
- Name of DrugDocument6 paginiName of DrugKathleen ColinioÎncă nu există evaluări
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDe la EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesEvaluare: 4 din 5 stele4/5 (2)
- Musculoskeletal System Disorders - Quiz #1 - 25 Questions - NurseslabsDocument35 paginiMusculoskeletal System Disorders - Quiz #1 - 25 Questions - Nurseslabswdnc98fgdyÎncă nu există evaluări
- 3 Osteosys DT Service Training EnglishDocument36 pagini3 Osteosys DT Service Training EnglishServicios Radiológicos s.a (SERASA)Încă nu există evaluări
- UK Clinical Guideline For The Prevention and Treatment of OsteoporosisDocument46 paginiUK Clinical Guideline For The Prevention and Treatment of OsteoporosisHninÎncă nu există evaluări
- Geochelone Pardalis) : Influence of The Calcium Content of The Diet Offered To Leopard Tortoises (Document5 paginiGeochelone Pardalis) : Influence of The Calcium Content of The Diet Offered To Leopard Tortoises (pzowtÎncă nu există evaluări
- Terapia Anabolica y Antiresortiva Secuencial en OsteoporosisDocument11 paginiTerapia Anabolica y Antiresortiva Secuencial en OsteoporosisTony Miguel Saba SabaÎncă nu există evaluări
- Nmt631bonedensitometry 161006214433Document19 paginiNmt631bonedensitometry 161006214433Noureddine BenarifaÎncă nu există evaluări
- Bone Mineral Densitometry Reporting Pearls and PitDocument16 paginiBone Mineral Densitometry Reporting Pearls and PitChon ChiÎncă nu există evaluări
- Article 324Document24 paginiArticle 324Kang ChenÎncă nu există evaluări
- Radiologic PathologyDocument11 paginiRadiologic PathologyElaiza IcazaÎncă nu există evaluări
- Pharmacotherapy Handbook 7th Edition-1-31-43Document13 paginiPharmacotherapy Handbook 7th Edition-1-31-43Erfin NingoÎncă nu există evaluări
- DOH Guideline For The Screening of OsteoporosisDocument11 paginiDOH Guideline For The Screening of OsteoporosisBasil al-hashaikehÎncă nu există evaluări
- Lunar Prodigy Primo: Simplicity and DedicationDocument4 paginiLunar Prodigy Primo: Simplicity and DedicationFernando OhashiÎncă nu există evaluări
- Continued Growth Hormone GH Treatment ADocument5 paginiContinued Growth Hormone GH Treatment AAnghel Ana-MariaÎncă nu există evaluări
- Novartis Osteoporosis Slide KitDocument42 paginiNovartis Osteoporosis Slide KitShravanti SatyanandÎncă nu există evaluări
- Osteoporosis Detection Using Machine and Deep Learning TechniquesDocument15 paginiOsteoporosis Detection Using Machine and Deep Learning TechniquesSeddik KhamousÎncă nu există evaluări
- SarcopeniaDocument16 paginiSarcopeniaNatalia Bernal RiquelmeÎncă nu există evaluări
- TMP E2 B6Document7 paginiTMP E2 B6FrontiersÎncă nu există evaluări
- (03241750 - Acta Medica Bulgarica) Antiretroviral Therapy and Bone HealthDocument6 pagini(03241750 - Acta Medica Bulgarica) Antiretroviral Therapy and Bone HealthTeodorÎncă nu există evaluări
- Dual Energy X-Ray Absorptiometry Body Composition Reference Values From NhanesDocument9 paginiDual Energy X-Ray Absorptiometry Body Composition Reference Values From NhanesJhonnyAndresBonillaHenaoÎncă nu există evaluări
- What Is Osteoporosis?Document6 paginiWhat Is Osteoporosis?MaryamÎncă nu există evaluări
- Horizon User Guide (MAN-04871) English Rev - 012 01-2020Document164 paginiHorizon User Guide (MAN-04871) English Rev - 012 01-2020colladoluzangelaÎncă nu există evaluări
- Mendelian Randomization Study of Inflammatory Bowel Disease and Bone Mineral DensityDocument19 paginiMendelian Randomization Study of Inflammatory Bowel Disease and Bone Mineral DensityYaumil ChoiriÎncă nu există evaluări
- AccuDEXA Model 7100 User GuideDocument82 paginiAccuDEXA Model 7100 User GuideManuel Vivero DiéguezÎncă nu există evaluări
- Pyrilinks D TestDocument5 paginiPyrilinks D TestandresÎncă nu există evaluări
- What Is Osteoporosis?: Osteoposis Is A Disease ofDocument48 paginiWhat Is Osteoporosis?: Osteoposis Is A Disease ofTaruna GargÎncă nu există evaluări
- Bio Project File 2Document19 paginiBio Project File 2jiya singhÎncă nu există evaluări
- Medical Physics Course Notes (Greg Pitt)Document92 paginiMedical Physics Course Notes (Greg Pitt)Mel ClancyÎncă nu există evaluări
- Ho Logic DR 4000Document8 paginiHo Logic DR 4000Félix Adilson ElíasÎncă nu există evaluări
- Quantum Healthcare Vietnam JSC: Global Support ofDocument48 paginiQuantum Healthcare Vietnam JSC: Global Support ofPhạm Nhật MinhÎncă nu există evaluări
- DXA Cross-Calibration InstructionsDocument3 paginiDXA Cross-Calibration InstructionslucasfullmetalÎncă nu există evaluări