Documente Academic
Documente Profesional
Documente Cultură
Epidemiologic Signatures in Cancer
Încărcat de
mariacarmenstoicaDrepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Epidemiologic Signatures in Cancer
Încărcat de
mariacarmenstoicaDrepturi de autor:
Formate disponibile
The n e w e ng l a n d j o u r na l of m e dic i n e
Spe ci a l R e p or t
Epidemiologic Signatures in Cancer
H. Gilbert Welch, M.D., M.P.H., Barnett S. Kramer, M.D., M.P.H., and William C. Black, M.D.
For more than a century, the United States has substantial disease reservoir of indolent, subclini-
devoted considerable effort to measuring the cal forms is particularly sensitive to the degree
population-based cancer burden. The effort be- of diagnostic scrutiny — the combined effect of
gan with the measurement of disease-specific the frequency of diagnostic or screening exam
mortality. The compilation of annual mortality inations (including the physical examination,
statistics began in 1900, and nationwide cover- imaging, and laboratory testing), the ability of
age was achieved in 1933.1 The measurement of the examinations to detect small irregularities,
incidence was understandably more challenging, and the threshold to label these as cancer. These
because it is easier to collect information about factors can lead to rapid, iatrogenic swings in
death than about diagnosis. The state of Con- reported incidence and conspire to make cancer
necticut initiated a population-based cancer reg- incidence an unreliable measure of true cancer
istry in 1935,2 and the National Cancer Institute occurrence.
established a national cancer registry in 1973 — In this article, we make use of 40 years of
the Surveillance, Epidemiology, and End Results data to examine patterns of incidence and mor-
(SEER) Program.3 tality for various cancers, following the intellec-
Over the years, another challenge has become tual lineage of Bailar and others.7-10 We go on to
apparent: observed cancer burden can be influ- posit what these epidemiologic signatures might
enced by diagnostic practice.4 New imaging and reveal about true cancer occurrence, overdiagno-
other diagnostic methods can allow a cancer sis, and treatment advances. By “true cancer oc-
diagnosis to be made earlier in the disease currence,” we mean the underlying incidence of
course, detect nodal and metastatic involvement clinically meaningful cancer (i.e., reported inci-
not recognized previously (shifting the stage of dence minus overdiagnosis) (see Glossary). We
cancer upward),5 and even reveal some cancers also consider the potential value of a variable
that would otherwise not become evident clini- that may serve as a marker for changes in true
cally — a phenomenon now referred to as over- cancer occurrence: the incidence of metastatic
diagnosis.6 The incidence of cancers that have a disease. We conclude by offering general princi-
Glossary
Mortality: The rate of death from a specific cause (or all causes combined) in a defined population in a given period.
Incidence: Although conventionally defined in terms of disease occurrence, reported incidence is actually the rate of dis-
ease diagnosis in a defined population in a given period.
Overdiagnosis: The diagnosis of cancers that would otherwise not become clinically evident — an unintended side ef-
fect of increased diagnostic scrutiny.
True cancer occurrence: The underlying incidence of clinically meaningful cancer (i.e., reported incidence minus overdi-
agnosis).
Clinically meaningful cancer: Cancer that would progress to cause symptoms and require treatment if left untreated and
put the patient at risk for premature death.
Metastatic incidence: The rate of cancer that is first diagnosed with metastases in a given period; its pattern over time
may be indicative of trends in true cancer occurrence.
1378 n engl j med 381;14 nejm.org October 3, 2019
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
Special Report
ples for interpreting signatures as well as sugges- currence; thus, the associated declining mortal-
tions for additional data that would allow for ity provides a clear signal of improvements in
more robust inferences. cancer treatment. The top graphs show the age-
adjusted absolute frequencies of incidence and
Appr oach mortality, whereas the bottom graphs show their
relative frequencies to the base year of 1975.
We examined mortality and incidence patterns In Hodgkin’s lymphoma, the gradual decline
from 1975 through 2015 for selected cancers in in mortality — juxtaposed with generally stable
the United States. Mortality data come from the incidence — reflects a steady improvement in
National Vital Statistics System maintained by treatment across time.11 In chronic myeloid leu-
the National Center for Health Statistics. Incidence kemia (CML), the mortality decline is much
data (combining invasive and in situ cancers) more precipitous, occurring in a narrow window
come from the original nine SEER registries: spanning the new millennium. This rapid de-
Atlanta, Connecticut, Detroit, Hawaii, Iowa, New cline coincides with the introduction of imatinib
Mexico, San Francisco–Oakland, Seattle–Puget and confirms that the agent was indeed a genuine
Sound, and Utah. breakthrough that was implemented rapidly into
For each cancer, we illustrated mortality and practice.12
incidence trends using a pair of graphics. The Figure 1B illustrates signatures consistent with
first depicts the absolute rates over time, age- a rise and fall in true cancer occurrence and
adjusted to the U.S. 2000 standard population. highlights the value of efforts to identify causal
The second depicts the relative rates over time, factors and eliminate them. Here, we focus on
in which the 1975 rate serves as the reference the cancer responsible for the most deaths in the
group. To dampen the volatility of less commonly United States (lung cancer, which caused more
occurring cancers, all incidence data were calcu- deaths than the next three cancers combined in
lated with the use of a 3-year running average. 201813) and examine the effect of the rise and
We also examined data on the incidence of fall of its most potent risk factor (cigarette
metastatic disease — a metric that includes only smoking).
cases in which cancer is first diagnosed when a In 1950, case–control studies by Wynder and
patient presents with metastases, not those in Graham in the United States14 and by Doll and
which early-stage cancer is diagnosed and then Hill in England15 identified cigarette smoking as
progresses to metastatic disease. These data are being strongly related to lung cancer. Six years
not recorded for the hematologic cancers and later, data from a prospective cohort assembled
were available only beginning in 1988 for lung by Doll and Hill showed that heavily smoking
and prostate cancer. Thus, for these two cancers, British physicians were 20 times more likely to
the relative rate of the incidence of metastatic die from lung cancer than were their nonsmok-
disease uses the 1988 rate as the referent group. ing colleagues.16 In 1964, U.S. Surgeon General
To illustrate potential divergent trends in overall Luther Terry confirmed that there was no doubt
incidence and in the incidence of metastatic that cigarette smoking caused lung cancer.17 The
disease in subsequent years, the relative rate of prevalence of ever smoking peaked during the
the incidence of metastatic disease in 1988 was 1950s among men; however, the peak was de-
set as equivalent to the relative rate of overall layed until the 1970s among women (ironically,
incidence in 1988 (1.14 for lung cancer in men, one of the effects of the women’s movement
1.95 for lung cancer in women, and 1.46 for during the late 1960s was the greater acceptabil-
prostate cancer) instead of 1.0. ity of smoking — something cigarette advertis-
ing quickly capitalized on).18,19 Because of the
different timing of exposure, we consider men
De sir a ble Signat ure s
and women separately.
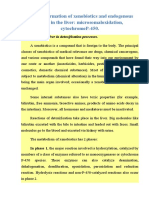
Figure 1 includes signatures readily understand- What is most striking about these signatures
able to clinicians. Figure 1A illustrates signatures is that incidence and mortality move together.
that reflect well on the value of medical care. For both sexes, the rise and fall of cigarette
Stable incidence signals stable true cancer oc- smoking is followed (approximately three decades
n engl j med 381;14 nejm.org October 3, 2019 1379
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
A
Hodgkin’s Lymphoma Chronic Myeloid Leukemia
2.0
3.0
Rate (per 100,000)
2.5 Incidence 1.5 Incidence
2.0
1.5 1.0
1.0
0.5 Mortality
Mortality
0.5
0.0 0.0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
1.2 1.2
Incidence Incidence
1.0 1.0
Rate Relative to 1975
0.8 0.8
0.6 0.6
0.4 Mortality 0.4 Mortality
0.2 0.2
0.0 0.0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
B
Lung Cancer in Men Lung Cancer in Women
100 60 Incidence
Incidence
Rate (per 100,000)
75 Mortality 45 Mortality
50 30
Metastatic incidence
25 15 Metastatic incidence
0 0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
1.4 2.5
Incidence Mortality
1.2
Rate Relative to 1975
Metastatic incidence 2.0 Incidence Metastatic
1.0 Mortality
incidence
0.8 1.5
0.6 1.0
0.4
0.5
0.2
0.0 0.0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
Figure 1. Readily Understandable Signatures.
Panel A shows improvements in treatment with stable true cancer occurrence. Panel B shows the rise and fall in
true cancer occurrence. Mortality is disease-specific — that is, the rate of death attributed to the specified cancer.
“Metastatic incidence” denotes the incidence of metastatic disease.
later) by a rise and fall in the occurrence of lung closely tracks incidence and mortality, its rela-
cancer. tive rate is slightly elevated in more recent years.
Figure 1B also includes the incidence of meta- This probably reflects upstaging, in which more
static disease: the rate at which persons receive intensive diagnostic evaluation and increasingly
a first diagnosis of cancer when they present sensitive tests are able to detect tiny metastases
with distant metastases. Although this metric not identified in earlier years — in this case,
1380 n engl j med 381;14 nejm.org October 3, 2019
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
Special Report
because of the growing use of positron-emission
tomography combined with computed tomog-
2015
2015
Incidence
Mortality
Mortality
raphy.20,21
Gradual diffusion
C Colorectal Cancer in Patients ≥50 Yr of Age, Screening
of screening
Figure 2 illustrates signatures that are argu-
ably the most desirable for society in general,
2005
2005
because they suggest that stomach, cervical, and
colorectal cancer are now simply less common
Initiated during Observation Period
than they were in 1975. The finding of incidence
1995
1995
and mortality declining at approximately the
Metastatic incidence
Metastatic incidence
same rate is consistent with declining true can-
1985 cer occurrence.
1985
Incidence These signatures also reflect the full range of
possible screening practices: from little or no
screening in stomach cancer to continuous
1975
1975
screening in cervical cancer, as well as an inter-
250
200
150
100
50
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Rate (per 100,000) Rate Relative to 1975 mediate screening condition in colorectal can-
cer. Thus, although the signatures are similar,
the underlying explanations for the decline may
differ. In stomach cancer, it is typically explained
2015
2015 by a decline in a powerful risk factor (Helicobacter
Metastatic incidence
Incidence
Mortality
pylori) perhaps related to increasing use of food
B Cervical Cancer in Women, Continuous Screening
preservatives, the dissemination of refrigeration,
2005
2005
or both.22 In cervical cancer, the decline is typi-
Mortality
cally explained by effective screening — the de-
tection and successful treatment of precancerous
1995
1995
throughout Observation Period
lesions.23
Metastatic incidence
Mortality is disease-specific — that is, the rate of death attributed to the specified cancer.
Because screening was initiated during the
period of observation, there is an opportunity to
1985
1985
see its effect in the colorectal-cancer signature
Incidence
(restricted to the commonly recommended tar-
Figure 2. Declining True Cancer Occurrence (with Variable Screening Practice).
get population for screening: patients ≥50 years
1975
1975
of age). There is no evidence of cancer overdiag-
16
12
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Rate (per 100,000) Rate Relative to 1975 nosis; in fact, incidence began to steadily decline
before widespread screening. Furthermore, the
incidence of metastatic disease and mortality
declined steadily throughout the period. Because
2015
2015
these trends predate screening (and because the
Incidence
Incidence
Mortality
Mortality
effect of early cancer detection and removal of
A Stomach Cancer, Little or No Screening throughout
precancerous lesions is necessarily delayed), this
2005
2005
signature reflects some decline in true cancer
occurrence in this age group that is unrelated to
screening.24
1995
1995
Metastatic incidence
Metastatic incidence
Unde sir a ble Signat ure s
1985
1985
Observation Period
As exemplified in the female lung-cancer signa-
ture before 2000, a concordant rise in incidence
and mortality is clearly undesirable. Figure 3
1975
1975
illustrates signatures that are instead discordant:
12
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Rate (per 100,000) Rate Relative to 1975 the reported incidence is rising, yet mortality is
stable. Stable mortality should be viewed as a
marker for stable true cancer occurrence. Although
n engl j med 381;14 nejm.org October 3, 2019 1381
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
it is possible that stable mortality could result
from a combination of increasing true cancer
2015
2015
Mortality
Mortality
occurrence and improvement in treatment, such
Incidence
Metastatic
incidence
a perfect annual counterbalancing of opposing
forces would be a remarkable coincidence.
2005
2005
Metastatic incidence
Incidence
Thus, the signatures for thyroid cancer, kid-
ney cancer, and melanoma suggest the detection
of cancers not destined to cause death: overdiag-
1995
1995
nosis. Although it is difficult to know which
persons are subject to overdiagnosis, overdiag-
nosis is easily appreciated at a population scale.
1985
1985
These signatures are undesirable because they
imply that more people are being told they have
cancer — and more are being treated for cancer
1975
1975
C Melanoma
— while true cancer occurrence remains stable.
50
40
30
20
10
6.0
5.0
4.0
3.0
2.0
1.0
Rate (per 100,000) Rate Relative to 1975 0.0 The additional finding of stable incidence of
metastatic disease further supports stable can-
cer occurrence. Although the small increases in
the incidence of metastatic thyroid cancer and
Metastatic incidence
2015
2015
melanoma observed in more recent years could
Mortality
Incidence
represent the onset of increasing cancer occur-
rence, they more likely reflect upstaging.
2005
2005
Signat ure s with Mixed Signal s
Incidence
1995
1995
Figure 4 illustrates the more complex epidemio-
Metastatic incidence
Mortality is disease-specific — that is, the rate of death attributed to the specified cancer.
logic signatures of breast and prostate cancer
Mortality
(restricted to women and men, respectively, ≥40
1985
1985
years of age) that present mixed effects: rising
incidence and falling mortality. Coincident with
B Kidney Cancer
the introduction of widespread screening mam-
1975
1975
mography, breast-cancer incidence increased rap-
16
12
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Rate (per 100,000) Rate Relative to 1975 idly and has apparently settled at a new, higher
baseline. This could represent either a substan-
tial (and focal) increase in true cancer occur-
Figure 3. Overdiagnosis with Stable True Cancer Occurrence.
rence or overdiagnosis associated with the intro-
2015
2015
Metastatic
incidence
duction of widespread screening. The relatively
Mortality
Metastatic incidence
stable incidence of metastatic disease, however,
favors the latter explanation. The decline in
2005
2005
mortality observed starting in the 1990s could
Incidence
reflect either improved treatment or screening or
Incidence
some combination of the two.25 Other data sug-
1995
1995
gest that improved treatment is the primary ex-
planation.26-30
Coincident with the introduction of wide-
1985
1985
spread prostate-specific antigen (PSA) screening,
Mortality
prostate-cancer incidence increased dramatically
A Thyroid Cancer
— yet has subsequently declined nearly to its
1975
1975
1975 baseline. This remarkable volatility cannot
15
12
3.0
2.5
2.0
1.5
1.0
0.5
0.0
Rate (per 100,000) Rate Relative to 1975 be explained by changes in true cancer occur-
rence. Instead, it highlights how sensitive pros-
tate cancer is to diagnostic scrutiny — in this
1382 n engl j med 381;14 nejm.org October 3, 2019
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
Special Report
A Breast Cancer in Women ≥40 Yr of Age B Prostate Cancer in Men ≥40 Yr of Age
Rate (per 100,000) 400 Incidence 500
Rate (per 100,000)
400 Incidence
300
300
200
200
100
Mortality 100 Mortality
Metastatic incidence Metastatic incidence
0 0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
Initiation of widespread
mammography Initiation of widespread
screening PSA screening
2.5 2.5
Incidence
Rate Relative to 1975
Rate Relative to 1975
2.0 2.0
Incidence
1.5 1.5
Metastatic incidence
1.0 1.0
Mortality
0.5 Mortality 0.5 Metastatic incidence
0.0 0.0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
Figure 4. Breast and Prostate Cancer.
Mortality is disease-specific — that is, the rate of death attributed to the specified cancer. PSA denotes prostate-
specific antigen.
A All Cancers, Men B All Cancers, Women
700
Incidence 500
600 Incidence
Rate (per 100,000)
Rate (per 100,000)
500 400
400 300
300
200
200
Mortality 100 Mortality
100
0 0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
1.4 Incidence 1.4
1.2 1.2 Incidence
Rate Relative to 1975
Rate Relative to 1975
1.0 1.0
0.8 0.8 Mortality
Mortality
0.6 0.6
0.4 0.4
0.2 0.2
0.0 0.0
1975 1985 1995 2005 2015 1975 1985 1995 2005 2015
Figure 5. All Cancers Combined.
Data are for male persons (Panel A) and female persons (Panel B) of all ages, but only 1% of cancers in both sexes
occur in persons younger than 20 years of age. Mortality refers to the rate of death attributed to all cancers com-
bined.
n engl j med 381;14 nejm.org October 3, 2019 1383
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
case, the breadth and frequency of PSA testing Gener al Principle s
and the PSA threshold that leads to a biopsy.31,32
The incidence of metastatic disease fell markedly The primary goals of this article are to enable
after the introduction of screening, which sug- general medical readers to interpret trends in
gests that screening does advance the time of the basic measures of population-based cancer
diagnosis for prostate cancers destined to become burden and to provide insight into true cancer
metastatic. It is important to reiterate, however, occurrence, overdiagnosis, and treatment ad-
that the incidence of metastatic disease includes vances. In particular, we encourage readers not
only cases in which cancer is first diagnosed to interpret cancer-incidence trends in isolation
when a patient presents with metastases (not — rather, interpret them in concert with trends
those in which early-stage cancer is diagnosed in cancer mortality, supplemented by trends
and then progresses to metastatic disease). Early in the incidence of metastatic disease, when
diagnosis and treatment of cancers that are des- available.
tined to manifest as metastases does not neces- There is little ambiguity when incidence is
sarily mean they will not ultimately go on to stable. A signature with both stable incidence
metastasize or cause death.33 Thus, the decline and stable mortality (not shown), as is roughly
in mortality that is observed starting in the the case for pancreatic and bladder cancer, sig-
1990s could reflect either improved treatment or nals little change in cancer occurrence and little
screening or some combination of the two. change in the effectiveness of treatment. A sig-
We would be remiss not to consider incidence nature with stable incidence and falling mortal-
and mortality for all cancers combined, as Bailar ity, in contrast, provides a strong signal of im-
did in 1986 and 1997.7,8 Our findings are shown proved treatment.
in Figure 5. In men, the volatile pattern of over- Changing incidence must be interpreted more
all incidence is clearly driven by prostate cancer, cautiously. When mirrored by mortality — that
which highlights how common the diagnosis is, incidence and mortality move in tandem —
became. The falling incidence in lung and colorec- changes in reported incidence should be viewed
tal cancer was canceled out by the rising inci- as changes in the underlying incidence of clini-
dence of melanoma and kidney cancer (a de- cally meaningful cancer (as exemplified in the
crease of 59 per 100,000 vs. an increase of 66 per lung-cancer signatures). A sustained increase in
100,000 between 1975 and 2015). incidence coupled with stable mortality, however,
Among women, rising overall cancer inci- suggests something fundamentally different: over-
dence during the 1980s predominantly reflects diagnosis superimposed on stable true cancer
the rising incidence of lung and breast cancer. occurrence.
The continued rise since the mid-1990s — de- More complex signatures are more challeng-
spite the falling incidence in colorectal, ovarian, ing and may be the result of multiple effects.
cervical, and, more recently, lung cancer — re- Increasing incidence and falling mortality could
flects the rising incidence of melanoma, kidney be the result of increased true cancer occurrence
cancer, and thyroid cancer (which is now three and improved treatment or, instead, overdiagno-
times as likely to be diagnosed in women as in sis (i.e., stable occurrence) and improved treat-
men, despite the fact that thyroid-cancer mortal- ment. Here, the incidence of metastatic disease
ity is the same among women and men34,35). may serve as an indicator of the change in true
Among both sexes, overall cancer mortality cancer occurrence.
has been falling since 1990. Among women, this Finally, rapid changes — those occurring
is largely driven by falling mortality from breast within several years — are best explained as the
cancer, colorectal cancer, and, more recently, effect of medical practice. Thus, the rapid decline
lung cancer. The more pronounced decline among in mortality from CML around 2000 and the
men reflects the more long-standing decline in rapid increase in breast-cancer incidence in the
lung-cancer mortality combined with declines 1980s reflect two dramatic changes in medical
in mortality from prostate cancer and colorectal practice attributable to distinct driving forces:
cancer. a genuine breakthrough in the treatment of CML
1384 n engl j med 381;14 nejm.org October 3, 2019
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
Special Report
and the widespread dissemination of mammo- istries about how to better capture system-level
graphic screening. effects.
In contrast, changing environmental expo- Critically, the ascertainment of incident can-
sures would typically exert their effect more cer cases should be accompanied by data on the
slowly. Consider the example of the widespread mode of cancer detection. Three broad catego-
exposure to one of the most powerful estab- ries could capture the driving force that led to
lished human carcinogens: tobacco smoke. The the cancer diagnosis: patient symptoms and signs
lung-cancer epidemic took decades to emerge (clinically detected), the systematic search for
and then additional decades to partially recede early cancer (screening-detected), or a chance
as smoking habits changed. The effects of chang- finding (incidentally detected). Distinguishing
es in germline inheritance (genetic drift) are among these three categories would further ex-
slower still, requiring generations to emerge. plain the origins of changes in reported inci-
dence. More relevant to physicians and patients,
data on the mode of detection also provide im-
Vir t ue of Simplicit y
portant prognostic information.
Admittedly, our epidemiologic-signatures approach Two additional pieces of information on can-
involves the simple interpretation of crude na- cer deaths would also be useful. First is the ex-
tional trends in two or three variables. By far the tent of disease at death: tumor size and stage
most important is cancer mortality, which re- — particularly data on whether metastases were
mains the single best measure of progress present. Second is data about the potential role
against cancer.36 Reported cancer incidence, on of treatment — specifically, whether the death
the other hand, should not be viewed as a reli- could have been related to treatment.
able measure of true cancer occurrence. Instead,
it must be interpreted in conjunction with mor- Conclusions
tality (and possibly the incidence of metastatic
disease) and knowledge about changing diag- Epidemiologic signatures that illustrate trends
nostic practice. in population-based data on cancer burden pro-
Efforts to add precision with complex statisti- vide insight into true cancer occurrence, over-
cal models typically involve multiple input vari- diagnosis, and treatment advances. They are im-
ables, which may emanate from select groups of portant indicators of the potential contribution
patients not representative of the population. of environmental exposures, primary preventive
Unstated assumptions (e.g., that reported inci- interventions, new treatments, and changing
dence equals true cancer occurrence) can inad- diagnostic and screening practices. Falling mor-
vertently introduce serious errors.37 Yet the valid- tality means that there has been real progress
ity of the input data and the effect of assumptions against cancer in the past 40 years — largely
are opaque to peer reviewers and clinicians (the reflecting improved treatment and the decline
“black box” problem), which makes it difficult of a uniquely powerful causal factor: cigarette
to apportion model outputs to changes in expo- smoking. The lack of an accompanying fall in
sure, treatment advances, or diagnostic shifts incidence is an unfortunate side effect of early
with confidence. cancer-detection efforts.
The opinions expressed in this article are those of the authors
and do not constitute official positions of the U.S. Government.
Need for Enhanced Data Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
The acquisition of population-based data on can- Dr. Welch thanks Ravinder Kang, M.D., for alerting him to the
cer burden is a fundamental attribute of a well- powerful effect of imatinib on mortality from chronic myeloid
leukemia while working as a teaching assistant in his under-
functioning health care system. So too is routine graduate course.
monitoring of these data to identify both envi-
ronmental and system effects. We believe these From the Center for Surgery and Public Health, Brigham and
Women’s Hospital, Boston (H.G.W.); the Division of Cancer
efforts warrant not only continued support but Control and Population Sciences, National Cancer Institute,
also creative thinking by cancer and death reg- Bethesda, MD (B.S.K.); and the Department of Radiology,
n engl j med 381;14 nejm.org October 3, 2019 1385
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
Special Report
Geisel School of Medicine at Dartmouth, Hanover, NH (W.C.B.). 19. Richmond R. You’ve come a long way baby: women and the
Address reprint requests to Dr. Welch at P.O. Box 114, Thetford, tobacco epidemic. Addiction 2003;98:553-7.
VT 05074, or at drgilwelch@gmail.com. 20. Dinan MA, Curtis LH, Carpenter WR, et al. Stage migration,
selection bias, and survival associated with the adoption of pos-
1. Historical development of cause of death statistics. Techni- itron emission tomography among Medicare beneficiaries with
cal paper 55. Bethesda, MD:International Institute for Vital Reg- non-small-cell lung cancer, 1998-2003. J Clin Oncol 2012;30:
istration and Statistics, September 1993 (https://www.cdc.gov/ 2725-30.
nchs/data/isp/055_historical_development_of_cause_of_death 21. Geiger GA, Kim MB, Xanthopoulos EP, et al. Stage migration
_stat.pdf). in planning PET/CT scans in patients due to receive radiotherapy
2. Haenszel W, Curnen MG. The first fifty years of the Con- for non-small-cell lung cancer. Clin Lung Cancer 2014;15:79-85.
necticut Tumor Registry: reminiscences and prospects. Yale J Biol 22. Fuchs CS, Mayer RJ. Gastric carcinoma. N Engl J Med 1995;
Med 1986;59:475-84. 333:32-41.
3. National Research Council, Committee on National Statis- 23. Cannistra SA, Niloff JM. Cancer of the uterine cervix. N Engl
tics. The U.S. Vital Statistics System: a national perspective. J Med 1996;334:1030-8.
Washington, DC:National Academies Press, 2009 (https://www 24. Welch HG, Robertson DJ. Colorectal cancer on the decline
.ncbi.nlm.nih.gov/books/NBK219884/). — why screening can’t explain it all. N Engl J Med 2016;374:
4. Black WC, Welch HG. Advances in diagnostic imaging and 1605-7.
overestimations of disease prevalence and the benefits of ther- 25. Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening
apy. N Engl J Med 1993;328:1237-43. and adjuvant therapy on mortality from breast cancer. N Engl J
5. Feinstein AR, Sosin DM, Wells CK. The Will Rogers phenom- Med 2005;353:1784-92.
enon: stage migration and new diagnostic techniques as a 26. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG).
source of misleading statistics for survival in cancer. N Engl J Med Effects of chemotherapy and hormonal therapy for early breast
1985;312:1604-8. cancer on recurrence and 15-year survival: an overview of the
6. Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer randomised trials. Lancet 2005;365:1687-717.
Inst 2010;102:605-13. 27. Blanks RG, Moss SM, McGahan CE, Quinn MJ, Babb PJ. Effect
7. Bailar JC III, Smith EM. Progress against cancer? N Engl J Med of NHS breast screening programme on mortality from breast
1986;314:1226-32. cancer in England and Wales, 1990-8: comparison of observed
8. Bailar JC III, Gornik HL. Cancer undefeated. N Engl J Med with predicted mortality. BMJ 2000;321:665-9.
1997;336:1569-74. 28. Kalager M, Zelen M, Langmark F, Adami HO. Effect of
9. Chu KC, Kramer BS, Smart CR. Analysis of the role of cancer screening mammography on breast-cancer mortality in Norway.
prevention and control measures in reducing cancer mortality. N Engl J Med 2010;363:1203-10.
J Natl Cancer Inst 1991;83:1636-43. 29. Bleyer A, Welch HG. Effect of three decades of screening
10. Cho H, Mariotto AB, Schwartz LM, Luo J, Woloshin S. When mammography on breast-cancer incidence. N Engl J Med 2012;
do changes in cancer survival mean progress? The insight from 367:1998-2005.
population incidence and mortality. J Natl Cancer Inst Monogr 30. Welch HG, Prorok PC, O’Malley AJ, Kramer BS. Breast-cancer
2014;49:187-97. tumor size, overdiagnosis, and mammography screening effec-
11. Kwan A, Chadwick N, Hancock B. Improving survival of pa- tiveness. N Engl J Med 2016;375:1438-47.
tients with Hodgkin lymphoma over 4 decades: experience of the 31. Negoita S, Feuer EJ, Mariotto A, et al. Annual report to the
British National Lymphoma Investigation (BNLI) with 6834 pa- nation on the status of cancer. II. Recent changes in prostate can-
tients. Clin Lymphoma Myeloma Leuk 2017;17:108-19. cer trends and disease characteristics. Cancer 2018;124:2801-14.
12. Longo DL. Imatinib changed everything. N Engl J Med 2017; 32. Welch HG, Brawley OW. Scrutiny-dependent cancer and self-
376:982-3. fulfilling risk factors. Ann Intern Med 2018;168:143-4.
13. Estimated new cancer cases and deaths for 2018. SEER Can- 33. Welch HG, Gorski DH, Albertsen PC. Trends in metastatic
cer Statistics Review 1975-2015 (https://seer.cancer.gov/csr/1975 breast and prostate cancer — lessons in cancer dynamics. N Engl
_2015/browse_csr.php?sectionSEL=1&pageSEL=sect_01_table.01). J Med 2015;373:1685-7.
14. Wynder EL, Graham EA. Tobacco smoking as a possible 34. American Cancer Society, Cancer Statistics Center. Thyroid
etiologic factor in bronchiogenic carcinoma: a study of 684 at a glance: incidence by sex. 2019 (https://cancerstatisticscenter
proved cases. J Am Med Assoc 1950;143:329-36. .cancer.org/cancer-site/Thyroid/dw1qthUo).
15. Doll R, Hill AB. Smoking and carcinoma of the lung: pre- 35. American Cancer Society, Cancer Statistics Center. Thyroid
liminary report. Br Med J 1950;2:739-48. at a glance: mortality by sex. 2019 (https://cancerstatisticscenter
16. Doll R, Hill AB. Lung cancer and other causes of death in .cancer.org/cancer-site/Thyroid/YDOaHk0C).
relation to smoking: a second report on the mortality of British 36. Extramural Committee to Assess Measures of Progress
doctors. Br Med J 1956;2:1071-81. Against Cancer. Measurement of progress against cancer. J Natl
17. Cigarettes peril health, U.S. report concludes: ‘remedial Cancer Inst 1990;82:825-35.
action’ urged: cancer link cited. New York Times. January 12, 37. Kramer BS, Elmore JG. Projecting the benefits and harms
1964:A1. of mammography using statistical models: proof or proofiness?
18. Holford TR, Meza R, Warner KE, et al. Tobacco control and J Natl Cancer Inst 2015;107(7):djv145.
the reduction in smoking-related premature deaths in the United DOI: 10.1056/NEJMsr1905447
States, 1964-2012. JAMA 2014;311:164-71. Copyright © 2019 Massachusetts Medical Society.
1386 n engl j med 381;14 nejm.org October 3, 2019
The New England Journal of Medicine
Downloaded from nejm.org on October 2, 2019. For personal use only. No other uses without permission.
Copyright © 2019 Massachusetts Medical Society. All rights reserved.
S-ar putea să vă placă și
- Transcendental Meditation and Treatment For Post-TraumaticDocument2 paginiTranscendental Meditation and Treatment For Post-TraumaticmariacarmenstoicaÎncă nu există evaluări
- Case Histories: Bipolar DisorderDocument1 paginăCase Histories: Bipolar DisordermariacarmenstoicaÎncă nu există evaluări
- Specific PhobiasDocument9 paginiSpecific PhobiasmariacarmenstoicaÎncă nu există evaluări
- GriegDocument7 paginiGriegmariacarmenstoica0% (1)
- Richard GallianoDocument3 paginiRichard Gallianomariacarmenstoica0% (1)
- Oral and Genital Ulcers in Behçet's Disease: Images in Clinical MedicineDocument1 paginăOral and Genital Ulcers in Behçet's Disease: Images in Clinical MedicinemariacarmenstoicaÎncă nu există evaluări
- Oboseala Final 229Document67 paginiOboseala Final 229mariacarmenstoicaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- MсKee's V.1 P.2 -2Document413 paginiMсKee's V.1 P.2 -2Jonnie Rose Louise WeeÎncă nu există evaluări
- TRIMBOW® 100/6/10 and 200/6/10: What Is in This Leaflet Before You Use TrimbowDocument6 paginiTRIMBOW® 100/6/10 and 200/6/10: What Is in This Leaflet Before You Use TrimbowShauna DunnÎncă nu există evaluări
- Febuxostat Vs AlopurinolDocument13 paginiFebuxostat Vs AlopurinolNilson Morales CordobaÎncă nu există evaluări
- Lecture 3 (Therapeutic Enzymes)Document14 paginiLecture 3 (Therapeutic Enzymes)daroshamchaudhary1237Încă nu există evaluări
- 1-3 Milestone One Topic ProposalDocument4 pagini1-3 Milestone One Topic Proposaljeffrey styerÎncă nu există evaluări
- K A HamiedDocument8 paginiK A HamiedArun GaderiyaÎncă nu există evaluări
- chapter-4-ACELLULAR AND PROKARYOTIK MICROBESDocument66 paginichapter-4-ACELLULAR AND PROKARYOTIK MICROBESCza Mae ArsenalÎncă nu există evaluări
- Starkville Dispatch Eedition 3-22-20Document20 paginiStarkville Dispatch Eedition 3-22-20The DispatchÎncă nu există evaluări
- Thrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Document39 paginiThrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Ericka SantosÎncă nu există evaluări
- Premalignant Lesions and Oral CancerDocument8 paginiPremalignant Lesions and Oral CancerKatelyn_FÎncă nu există evaluări
- WJD 2 196 PDFDocument8 paginiWJD 2 196 PDFMayra PereiraÎncă nu există evaluări
- Periapical DiseasesDocument31 paginiPeriapical DiseasesKhaled ElshabrawyÎncă nu există evaluări
- Bawasig Pediatric ExamDocument20 paginiBawasig Pediatric Examخلدون سليمÎncă nu există evaluări
- Biotransfermation of XenobioticsDocument34 paginiBiotransfermation of XenobioticsМохіт Кумар ЯмпатіÎncă nu există evaluări
- Exam 3Document14 paginiExam 31glimpseÎncă nu există evaluări
- Daftar PustakaDocument6 paginiDaftar PustakaVERTEBRAE COASSÎncă nu există evaluări
- Biosafety and Biosecurity 1Document3 paginiBiosafety and Biosecurity 1JEUEL DYLAN DINSAYÎncă nu există evaluări
- No. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Document12 paginiNo. 10 SANAANI Topic For Esophagogastric Balloon Tamponade Tubes Billroth 1 and 11Nur SanaaniÎncă nu există evaluări
- Full Download Textbook of Diagnostic Microbiology 6th Edition Mahon Test BankDocument35 paginiFull Download Textbook of Diagnostic Microbiology 6th Edition Mahon Test Bankisaaccastrole100% (32)
- Diabetes Infographics by SlidesgoDocument33 paginiDiabetes Infographics by SlidesgoМария ТоневаÎncă nu există evaluări
- Clasificación Endo-PerioDocument4 paginiClasificación Endo-PerioJonathan SanchezÎncă nu există evaluări
- Draft Nepra Hse Code 2021Document68 paginiDraft Nepra Hse Code 2021Syed Fawad ShahÎncă nu există evaluări
- Clauneta MondlaneDocument7 paginiClauneta MondlaneMiguelOriellÎncă nu există evaluări
- Liver and Gallbladder Acquired Authority by Rosina Sonnenschmidt Reading ExtractDocument11 paginiLiver and Gallbladder Acquired Authority by Rosina Sonnenschmidt Reading ExtractSohail Latif100% (1)
- Bacteriology - Semifinals - Neisseria and MoraxellaDocument10 paginiBacteriology - Semifinals - Neisseria and MoraxellaUshuaia Ira Marie L. GallaronÎncă nu există evaluări
- Copy p1 Week 5 Nur 098 ActivityDocument5 paginiCopy p1 Week 5 Nur 098 ActivityRomelyn DellezoÎncă nu există evaluări
- Dr. Adrian Marinescu Matei Bals Virgil Musta, Medic Primar de Boli InfecțioaseDocument17 paginiDr. Adrian Marinescu Matei Bals Virgil Musta, Medic Primar de Boli InfecțioaseDragosAurÎncă nu există evaluări
- Amebiasis ReportDocument58 paginiAmebiasis ReportdoreenÎncă nu există evaluări
- Severe Acute Malnutrition - MSF Medical GuidelinesDocument6 paginiSevere Acute Malnutrition - MSF Medical GuidelinesAnas AdamuÎncă nu există evaluări
- Microbicidal Effect of Embilica Officianalis On Black Pigmented Bacteria in Patients With Periimplant MucositisDocument10 paginiMicrobicidal Effect of Embilica Officianalis On Black Pigmented Bacteria in Patients With Periimplant MucositisARAVINDAN GEETHA KRRISHNANÎncă nu există evaluări