S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- EXCI360 Chapter 75Document19 paginiEXCI360 Chapter 75jessÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Project Management A Technicians Guide Staples TOCDocument5 paginiProject Management A Technicians Guide Staples TOCAnonymous NwnJNO0% (3)
- Management of Preterm LaborDocument2 paginiManagement of Preterm LaborpolygoneÎncă nu există evaluări
- FEM 3004 - Lab 10 Part 2editedDocument26 paginiFEM 3004 - Lab 10 Part 2editedAINA NADHIRAH BINTI A ROZEY / UPMÎncă nu există evaluări
- Scope: Procter and GambleDocument30 paginiScope: Procter and GambleIrshad AhamedÎncă nu există evaluări
- Medical Records in Family PracticeDocument22 paginiMedical Records in Family PracticenurfadillahÎncă nu există evaluări
- EXCI360 Ch80 Notes 2019-2020Document15 paginiEXCI360 Ch80 Notes 2019-2020jessÎncă nu există evaluări
- Class Activity 1Document1 paginăClass Activity 1jessÎncă nu există evaluări
- REVISED EXCI 360 Course Outline W2020 PDFDocument9 paginiREVISED EXCI 360 Course Outline W2020 PDFjessÎncă nu există evaluări
- 3-Vestibular System Part 2 - StudentsDocument18 pagini3-Vestibular System Part 2 - StudentsjessÎncă nu există evaluări
- EXCI-360 UpperMotorNeuron 2020Document35 paginiEXCI-360 UpperMotorNeuron 2020jessÎncă nu există evaluări
- 4-Visual System - StudentsDocument18 pagini4-Visual System - StudentsjessÎncă nu există evaluări
- EXCI-360 LowerMN 2020Document30 paginiEXCI-360 LowerMN 2020jessÎncă nu există evaluări
- 3-Vestibular System Part 1 - StudentsDocument22 pagini3-Vestibular System Part 1 - StudentsjessÎncă nu există evaluări
- EXCI360 Ch77 Notes 2019-20Document16 paginiEXCI360 Ch77 Notes 2019-20jessÎncă nu există evaluări
- EXCI-360 Cerebellum 2020Document25 paginiEXCI-360 Cerebellum 2020jessÎncă nu există evaluări
- 4-Visual System - StudentsDocument18 pagini4-Visual System - StudentsjessÎncă nu există evaluări
- 3-Vestibular System Part 2 - StudentsDocument18 pagini3-Vestibular System Part 2 - StudentsjessÎncă nu există evaluări
- EXCI-360 BasalGanglia 2020Document29 paginiEXCI-360 BasalGanglia 2020jessÎncă nu există evaluări
- 1-Somatosensory System - StudentsDocument20 pagini1-Somatosensory System - StudentsjessÎncă nu există evaluări
- 2-Pain StudentsDocument36 pagini2-Pain StudentsjessÎncă nu există evaluări
- EXCI360 Ch79 Notes 2019-20Document18 paginiEXCI360 Ch79 Notes 2019-20jessÎncă nu există evaluări
- EXCI360 Ch78 Notes 2019-20Document16 paginiEXCI360 Ch78 Notes 2019-20jessÎncă nu există evaluări
- EXCI360 Ch76 Notes 2019-20Document13 paginiEXCI360 Ch76 Notes 2019-20jessÎncă nu există evaluări
- EXCI360 Ch76 Notes ADH 2019 - 20Document6 paginiEXCI360 Ch76 Notes ADH 2019 - 20jessÎncă nu există evaluări
- EXCI360 Ch75 Full Notes 2019-20Document11 paginiEXCI360 Ch75 Full Notes 2019-20jessÎncă nu există evaluări
- Castle 1-3K E ManualDocument26 paginiCastle 1-3K E ManualShami MudunkotuwaÎncă nu există evaluări
- Adenoid HypertrophyDocument56 paginiAdenoid HypertrophyWidi Yuli HariantoÎncă nu există evaluări
- Chapter 2 and 3 ImmunologyDocument16 paginiChapter 2 and 3 ImmunologyRevathyÎncă nu există evaluări
- Neopuff PDFDocument4 paginiNeopuff PDFoechimÎncă nu există evaluări
- User ManualDocument21 paginiUser ManualKali PrasadÎncă nu există evaluări
- Neurocisticercosis PDFDocument7 paginiNeurocisticercosis PDFFiorella Alexandra HRÎncă nu există evaluări
- Study Notes On Isomers and Alkyl HalidesDocument3 paginiStudy Notes On Isomers and Alkyl HalidesChristian Josef AvelinoÎncă nu există evaluări
- Registration Statement (For Single Proprietor)Document2 paginiRegistration Statement (For Single Proprietor)Sherwin SalanayÎncă nu există evaluări
- 208-Audit Checklist-Autoclave Operation - FinalDocument6 pagini208-Audit Checklist-Autoclave Operation - FinalCherry Hope MistioÎncă nu există evaluări
- IsoTherming® Hydroprocessing TechnologyDocument4 paginiIsoTherming® Hydroprocessing Technologyromi moriÎncă nu există evaluări
- Contractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountDocument1 paginăContractor: Item No. MRS-1st 2021 Ref. Description Unit Quantity Rate of Contractor Unit Rate in Words AmountusmanaliÎncă nu există evaluări
- Engineering Project ListDocument25 paginiEngineering Project ListSyed ShaÎncă nu există evaluări
- "Next Friend" and "Guardian Ad Litem" - Difference BetweenDocument1 pagină"Next Friend" and "Guardian Ad Litem" - Difference BetweenTeh Hong Xhe100% (2)
- Thanks For Visiting Our Page!: Hi Doc!Document15 paginiThanks For Visiting Our Page!: Hi Doc!bey luÎncă nu există evaluări
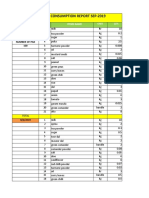
- Daily Staff Food Consumption Reports Sep-2019Document4 paginiDaily Staff Food Consumption Reports Sep-2019Manjit RawatÎncă nu există evaluări
- University of Puerto Rico at PonceDocument16 paginiUniversity of Puerto Rico at Ponceapi-583167359Încă nu există evaluări
- ZX110to330 ELEC E PDFDocument1 paginăZX110to330 ELEC E PDFYadi100% (1)
- Bacterial Genome Assembly IlluminaDocument49 paginiBacterial Genome Assembly IlluminadksaÎncă nu există evaluări
- 2 Dawn150Document109 pagini2 Dawn150kirubelÎncă nu există evaluări
- Psychoanalysis AND History: Freud: Dreaming, Creativity and TherapyDocument2 paginiPsychoanalysis AND History: Freud: Dreaming, Creativity and TherapyJuan David Millán MendozaÎncă nu există evaluări
- BQ - Electrical Calibration Relay Bld803, NPBDocument2 paginiBQ - Electrical Calibration Relay Bld803, NPBKazuya KasumiÎncă nu există evaluări
- A Critical Appreciation of Ode To NightingaleDocument3 paginiA Critical Appreciation of Ode To NightingaleBaloch Karawan100% (2)
- Crime Data Analysis 1Document2 paginiCrime Data Analysis 1kenny laroseÎncă nu există evaluări
- Not Really A StoryDocument209 paginiNot Really A StorySwapnaÎncă nu există evaluări
- Case Study of Milk ProductionDocument46 paginiCase Study of Milk Productionmian21100% (2)