S-ar putea să vă placă și
- Lobar AtelectasisDocument9 paginiLobar AtelectasisGusti Ngurah PÎncă nu există evaluări
- Contrast Media and The Kidney European Society ofDocument6 paginiContrast Media and The Kidney European Society ofdrrahulsshindeÎncă nu există evaluări
- Imaging Features of Pelvic EndometriosisDocument7 paginiImaging Features of Pelvic EndometriosisdrrahulsshindeÎncă nu există evaluări
- Sister Mary Joseph NoduleDocument4 paginiSister Mary Joseph NoduledrrahulsshindeÎncă nu există evaluări
- Spinal Ultrasound in InfantsDocument9 paginiSpinal Ultrasound in InfantsdrrahulsshindeÎncă nu există evaluări
- Female Genital Tuberculosis HysterosalpingiographyDocument6 paginiFemale Genital Tuberculosis HysterosalpingiographydrrahulsshindeÎncă nu există evaluări
- Soft Tissue Tumours and Mass-Like Lesions of The Chest WallDocument7 paginiSoft Tissue Tumours and Mass-Like Lesions of The Chest WalldrrahulsshindeÎncă nu există evaluări
- CT Main Pulm Art DiameterDocument3 paginiCT Main Pulm Art DiameterdrrahulsshindeÎncă nu există evaluări
- Scrotal Calci CationDocument6 paginiScrotal Calci CationdrrahulsshindeÎncă nu există evaluări
- Colour Doppler Ultrasound Ow Patterns in The Portal VeinDocument11 paginiColour Doppler Ultrasound Ow Patterns in The Portal VeindrrahulsshindeÎncă nu există evaluări
- Vesicoureteric Reflux in The AdultDocument9 paginiVesicoureteric Reflux in The AdultdrrahulsshindeÎncă nu există evaluări
- Ultrasound Evaluation of The Brosis Stage in Chronic LiverDocument9 paginiUltrasound Evaluation of The Brosis Stage in Chronic LiverdrrahulsshindeÎncă nu există evaluări
- Imaging of The Petrous ApexDocument9 paginiImaging of The Petrous ApexdrrahulsshindeÎncă nu există evaluări
- Ultrasound Spectrum of Intraductal Papillary NeoplasmsDocument7 paginiUltrasound Spectrum of Intraductal Papillary NeoplasmsdrrahulsshindeÎncă nu există evaluări
- Trigeminal Nerve Anatomy and PathologyDocument10 paginiTrigeminal Nerve Anatomy and PathologydrrahulsshindeÎncă nu există evaluări
- CT of Duodenal PathologyDocument7 paginiCT of Duodenal PathologydrrahulsshindeÎncă nu există evaluări
- Trigeminal Nerve Anatomy and PathologyDocument10 paginiTrigeminal Nerve Anatomy and PathologydrrahulsshindeÎncă nu există evaluări
- Cancer Risks From Diagnostic RadiologyDocument17 paginiCancer Risks From Diagnostic RadiologydrrahulsshindeÎncă nu există evaluări
- CT of A Thickened-Wall Gall BladderDocument7 paginiCT of A Thickened-Wall Gall BladderdrrahulsshindeÎncă nu există evaluări
- CT of Thoracic Lymph Nodes AnatomyDocument7 paginiCT of Thoracic Lymph Nodes AnatomydrrahulsshindeÎncă nu există evaluări
- Contrast Media and The Kidney European Society ofDocument6 paginiContrast Media and The Kidney European Society ofdrrahulsshindeÎncă nu există evaluări
- Imaging Features of Pelvic EndometriosisDocument7 paginiImaging Features of Pelvic EndometriosisdrrahulsshindeÎncă nu există evaluări
- CT Scanning of Middle Ear CholesteatomaDocument6 paginiCT Scanning of Middle Ear CholesteatomadrrahulsshindeÎncă nu există evaluări
- Cancer Risks From Diagnostic RadiologyDocument17 paginiCancer Risks From Diagnostic RadiologydrrahulsshindeÎncă nu există evaluări
- Surgical Anatomy PF PNSDocument11 paginiSurgical Anatomy PF PNSdrrahulsshindeÎncă nu există evaluări
- Radiographic Assessment of CTEVDocument6 paginiRadiographic Assessment of CTEVdrrahulsshindeÎncă nu există evaluări
- Tubeless Hypotonic DuodenographyDocument12 paginiTubeless Hypotonic DuodenographydrrahulsshindeÎncă nu există evaluări
- CT Findings in Pulmonary TuberculosisDocument13 paginiCT Findings in Pulmonary TuberculosisdrrahulsshindeÎncă nu există evaluări
- Multiplanar Sinus CT AJRDocument10 paginiMultiplanar Sinus CT AJRdrrahulsshindeÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5782)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Aerogard Tropical Strength Personal InsectDocument9 paginiAerogard Tropical Strength Personal Insectdavmac79Încă nu există evaluări
- Uma Kita.: Skylite Musicals 2019 Visual AtmosphereDocument14 paginiUma Kita.: Skylite Musicals 2019 Visual AtmosphereJasmine AyuÎncă nu există evaluări
- MSDS MnO2Document6 paginiMSDS MnO2fajarismanadiaÎncă nu există evaluări
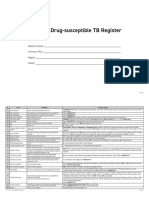
- Form 6a. Drug Susceptible TB RegisterDocument4 paginiForm 6a. Drug Susceptible TB RegisterAllen ChesterÎncă nu există evaluări
- Diet Ant PDFDocument3 paginiDiet Ant PDFAnonymous ZvBtfvÎncă nu există evaluări
- Rorschach TestDocument20 paginiRorschach TestEldho SabuÎncă nu există evaluări
- Toward Understanding Understanding: The Importance of Feeling Understood in RelationshipsDocument22 paginiToward Understanding Understanding: The Importance of Feeling Understood in RelationshipsevelyneÎncă nu există evaluări
- Art 5Document28 paginiArt 5sheheryar.sixsigmatravelsÎncă nu există evaluări
- Island in A Sea of SolitudeDocument4 paginiIsland in A Sea of SolitudeRuth BergerÎncă nu există evaluări
- Republic V Cagandahan DigestDocument2 paginiRepublic V Cagandahan DigestJustin Paras100% (1)
- Receiving Faculty Approval For The Following:: WWW - Aut.ac - Nz/health-AddendumDocument2 paginiReceiving Faculty Approval For The Following:: WWW - Aut.ac - Nz/health-AddendumsajithzxÎncă nu există evaluări
- European Guidelines On DRLs For Paediatric Imaging PDFDocument105 paginiEuropean Guidelines On DRLs For Paediatric Imaging PDFPapadoveÎncă nu există evaluări
- Biodiversity and A Healthy Society: Group 2Document14 paginiBiodiversity and A Healthy Society: Group 2Dianna Lynn MolinaÎncă nu există evaluări
- Nursing Care Plan GuideDocument1 paginăNursing Care Plan GuideJan Oliver YaresÎncă nu există evaluări
- NUR5020-James AxisaDocument204 paginiNUR5020-James AxisaVicky Torina ShilohÎncă nu există evaluări
- The Belly Fat Diet John ChathamDocument92 paginiThe Belly Fat Diet John ChathamGurpreet Kaur100% (3)
- #14 Overhead WorkDocument1 pagină#14 Overhead WorkAchmad MahatdzirÎncă nu există evaluări
- Capstone Project 1 ProposalDocument3 paginiCapstone Project 1 ProposalAnis ShatnawiÎncă nu există evaluări
- Joint Response by Texas HHSC, DFPS To CWOP Expert Panel RecommendationsDocument9 paginiJoint Response by Texas HHSC, DFPS To CWOP Expert Panel RecommendationsdmnpoliticsÎncă nu există evaluări
- MSDS-POLINTEK L & P Group-DMI INDUSTRIDocument8 paginiMSDS-POLINTEK L & P Group-DMI INDUSTRIYosep SasadaÎncă nu există evaluări
- MushroomsDocument64 paginiMushroomsHervis FantiniÎncă nu există evaluări
- Dow Integraflux™ Ultrafiltration Modules: Product Data SheetDocument3 paginiDow Integraflux™ Ultrafiltration Modules: Product Data SheetArunkumar ChandaranÎncă nu există evaluări
- Intramuscular Injection (Lidocain 4ml and Flamicort 40 MG) For Patient With Piriformis SyndromeDocument7 paginiIntramuscular Injection (Lidocain 4ml and Flamicort 40 MG) For Patient With Piriformis SyndromeLAKSMIÎncă nu există evaluări
- Condensable PM Issues-Ron MyersDocument16 paginiCondensable PM Issues-Ron MyersRachel JenkinsÎncă nu există evaluări
- SARS-CoV-2 Test Negative for 13-Year-Old MaleDocument3 paginiSARS-CoV-2 Test Negative for 13-Year-Old MaleBCom HonsÎncă nu există evaluări
- Short Answer Type QuestionsDocument3 paginiShort Answer Type QuestionsDhiman DeyÎncă nu există evaluări
- Tarlac State University Nursing Students Achieve Level III AccreditationDocument10 paginiTarlac State University Nursing Students Achieve Level III AccreditationBethrice MelegritoÎncă nu există evaluări
- Force-Feeding in Mauritania, Shanyah McCluneyDocument8 paginiForce-Feeding in Mauritania, Shanyah McCluneyShanyah McCluneyÎncă nu există evaluări
- Personal Employability Profile AssignmentDocument3 paginiPersonal Employability Profile Assignmentapi-490232390Încă nu există evaluări
- Taryn ZadunayskiDocument2 paginiTaryn Zadunayskiapi-278580762Încă nu există evaluări