S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Water Systems Report - Part4Document14 paginiWater Systems Report - Part4alang_businessÎncă nu există evaluări
- Ghaneeizad (2013)Document25 paginiGhaneeizad (2013)alang_businessÎncă nu există evaluări
- Biosand Filter Manual: Design, Construction, Installation, Operation and MaintenanceDocument94 paginiBiosand Filter Manual: Design, Construction, Installation, Operation and Maintenancealang_businessÎncă nu există evaluări
- Mixing Science and Practice A Reflective View FinalDocument62 paginiMixing Science and Practice A Reflective View Finalalang_businessÎncă nu există evaluări
- Safety Data Sheet: Magnafloc LT25Document9 paginiSafety Data Sheet: Magnafloc LT25alang_businessÎncă nu există evaluări
- Subramani - Numerical Analysis On Horizontal Jet FlocculatesDocument6 paginiSubramani - Numerical Analysis On Horizontal Jet Flocculatesalang_businessÎncă nu există evaluări
- Biosand Filter CAWST Part6Document10 paginiBiosand Filter CAWST Part6alang_businessÎncă nu există evaluări
- Appendix O: Sand Sieve AnalysisDocument4 paginiAppendix O: Sand Sieve Analysisalang_businessÎncă nu există evaluări
- Place The Media: Appendix FDocument10 paginiPlace The Media: Appendix Falang_businessÎncă nu există evaluări
- Appendix G: Filter Construction ChecklistDocument10 paginiAppendix G: Filter Construction Checklistalang_businessÎncă nu există evaluări
- Figure 9: Very Turbid Water in The Abstraction Well of A HafirDocument8 paginiFigure 9: Very Turbid Water in The Abstraction Well of A Hafiralang_businessÎncă nu există evaluări
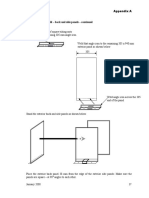
- Step 11: Exterior Mold - Back and Side Panels - Continued: Appendix ADocument10 paginiStep 11: Exterior Mold - Back and Side Panels - Continued: Appendix Aalang_businessÎncă nu există evaluări
- Interior Side Pieces, Bottom (4 Pieces) : Step 2: Layout and Cut 6.4 MM ( ") Steel PlateDocument10 paginiInterior Side Pieces, Bottom (4 Pieces) : Step 2: Layout and Cut 6.4 MM ( ") Steel Platealang_businessÎncă nu există evaluări
- Biosand Filter CAWST Part2 PDFDocument10 paginiBiosand Filter CAWST Part2 PDFalang_businessÎncă nu există evaluări
- Biosand Filter CAWST Part3 PDFDocument10 paginiBiosand Filter CAWST Part3 PDFalang_businessÎncă nu există evaluări
- Technical Guidelines For The Construction and Management of Improved HafirsDocument8 paginiTechnical Guidelines For The Construction and Management of Improved Hafirsalang_businessÎncă nu există evaluări
- Bio-Sand Filtration Filter Casting Instructions: United Kingdom MadagascarDocument4 paginiBio-Sand Filtration Filter Casting Instructions: United Kingdom Madagascaralang_businessÎncă nu există evaluări
- Biosand Filter Manual: Design, Construction, Installation, Operation and MaintenanceDocument10 paginiBiosand Filter Manual: Design, Construction, Installation, Operation and Maintenancealang_businessÎncă nu există evaluări
- Step 2 - Greasing and Assembling The Mould:: Bio-Sand Filter Construction Guidelines Page 5 of 10Document4 paginiStep 2 - Greasing and Assembling The Mould:: Bio-Sand Filter Construction Guidelines Page 5 of 10alang_businessÎncă nu există evaluări
- Annex 2: The Development of These Technical GuidelinesDocument8 paginiAnnex 2: The Development of These Technical Guidelinesalang_businessÎncă nu există evaluări
- Design Procedures of Improved HafirsDocument8 paginiDesign Procedures of Improved Hafirsalang_businessÎncă nu există evaluări
- Bio-Sand Filter Construction Guidelines Page 9 of 10Document2 paginiBio-Sand Filter Construction Guidelines Page 9 of 10alang_businessÎncă nu există evaluări
- Membranes 09 00111Document81 paginiMembranes 09 00111alang_businessÎncă nu există evaluări
- NSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part5Document8 paginiNSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part5alang_businessÎncă nu există evaluări
- Unit of Flocculant Dosing Set, Clarifier) : To Livestock WateringDocument8 paginiUnit of Flocculant Dosing Set, Clarifier) : To Livestock Wateringalang_businessÎncă nu există evaluări
- NSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part4Document8 paginiNSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part4alang_businessÎncă nu există evaluări
- 2018 Drinking Water Chlorination Booklet - Part5Document7 pagini2018 Drinking Water Chlorination Booklet - Part5alang_businessÎncă nu există evaluări
- NSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part2Document8 paginiNSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part2alang_businessÎncă nu există evaluări
- NSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part3Document8 paginiNSS (2011) SHTM 04-01 Part F Chloramination of Water Supplies - Part3alang_businessÎncă nu există evaluări
- 2018 Drinking Water Chlorination Booklet - Part4Document7 pagini2018 Drinking Water Chlorination Booklet - Part4alang_businessÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Assignment in FAMCOMDocument1 paginăAssignment in FAMCOMFeyre LunaÎncă nu există evaluări
- 10 Tips For HospitalsDocument2 pagini10 Tips For HospitalsVasu KodagantiÎncă nu există evaluări
- Infection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementDocument125 paginiInfection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementZhu Chen ChuanÎncă nu există evaluări
- Nursing Informatics: Master of Arts in NursingDocument3 paginiNursing Informatics: Master of Arts in NursingMaica LectanaÎncă nu există evaluări
- PratikPatel - Duodenal AtresiaDocument1 paginăPratikPatel - Duodenal AtresiaIkhlasia Amali MahzumÎncă nu există evaluări
- Physical Therapy Skills ChecklistDocument3 paginiPhysical Therapy Skills ChecklistnorthweststaffingÎncă nu există evaluări
- Table A13 - PMH PSH Meds Allergies FHX SohxDocument1 paginăTable A13 - PMH PSH Meds Allergies FHX SohxDragutin PetrićÎncă nu există evaluări
- Basic Measurements in EpidemiologyDocument58 paginiBasic Measurements in EpidemiologyRida AwwalÎncă nu există evaluări
- Phrp-Activity-Training CertificateDocument119 paginiPhrp-Activity-Training Certificateapi-247959633Încă nu există evaluări
- OPPE-FPPE ToolkitDocument71 paginiOPPE-FPPE ToolkitHosi Pba100% (1)
- CDC Booster RecommendationsDocument21 paginiCDC Booster RecommendationsNational Content DeskÎncă nu există evaluări
- (DR Schuster, Nykolyn) Communication For Nurses H (BookFi)Document215 pagini(DR Schuster, Nykolyn) Communication For Nurses H (BookFi)Ariefatun Nisa100% (1)
- Tubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSDocument12 paginiTubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSAulia PuspitaÎncă nu există evaluări
- 2018 Onychomycosis. Epidemiology, Clinical Features, and Diagnosis. UPTODATEDocument29 pagini2018 Onychomycosis. Epidemiology, Clinical Features, and Diagnosis. UPTODATEJoseloÎncă nu există evaluări
- Medical Service Citizen's Charter FY 2023Document12 paginiMedical Service Citizen's Charter FY 2023admin OESPAÎncă nu există evaluări
- Molecular Diagnostics: Report Status - Final Test Name Result Biological Ref. Interval UnitDocument2 paginiMolecular Diagnostics: Report Status - Final Test Name Result Biological Ref. Interval UnitAryan RathoreÎncă nu există evaluări
- QR Management of Breast Cancer (3rd Ed)Document8 paginiQR Management of Breast Cancer (3rd Ed)Jye yiÎncă nu există evaluări
- Systemic Inflammatory Response Syndrome (SIRS) PrognosisDocument16 paginiSystemic Inflammatory Response Syndrome (SIRS) PrognosisIPGDx100% (1)
- Philippine Health Care Delivery SystemDocument10 paginiPhilippine Health Care Delivery SystemKristel AnneÎncă nu există evaluări
- Notice: Organization, Functions, and Authority Delegations: Office of Public Health Emergency PreparednessDocument2 paginiNotice: Organization, Functions, and Authority Delegations: Office of Public Health Emergency PreparednessJustia.comÎncă nu există evaluări
- Practice - English Lesson - Fira Yuniar - 200704009Document5 paginiPractice - English Lesson - Fira Yuniar - 200704009Fira YuniarÎncă nu există evaluări
- History of Medical Technology in The USDocument8 paginiHistory of Medical Technology in The USMark justine GamiaoÎncă nu există evaluări
- College of Health Sciences: Kabacan, Cotabato PhilippinesDocument2 paginiCollege of Health Sciences: Kabacan, Cotabato PhilippinesKervy JuntillaÎncă nu există evaluări
- Indian Women and Health Related IssuesDocument29 paginiIndian Women and Health Related Issuesuma_mandeÎncă nu există evaluări
- Nurse Writing 003 OET Practice Letter by PASS OETDocument3 paginiNurse Writing 003 OET Practice Letter by PASS OETTwila Abuedo78% (9)
- COMSATS University Islamabad HUM102 Report Writing Skills Assignment # 2 Fall 2020Document3 paginiCOMSATS University Islamabad HUM102 Report Writing Skills Assignment # 2 Fall 2020Abdul WahabÎncă nu există evaluări
- Management of Preterm LaborDocument2 paginiManagement of Preterm LaborpolygoneÎncă nu există evaluări
- Amoxil: Amoxil Capsules 250 MG and 500 MG AmoxicillinDocument6 paginiAmoxil: Amoxil Capsules 250 MG and 500 MG AmoxicillinNaimat Ullah MuhammadÎncă nu există evaluări
- ATLS PretestDocument3 paginiATLS PretestDavid Reznick100% (5)
- Foreign RRL and SDocument4 paginiForeign RRL and SAlthea SaguinsinÎncă nu există evaluări