S-ar putea să vă placă și
- A Guide to District Court Civil Forms in the State of HawaiiDe la EverandA Guide to District Court Civil Forms in the State of HawaiiÎncă nu există evaluări
- Stipulations With Request For AwardDocument9 paginiStipulations With Request For Awardlynnedeguzman944Încă nu există evaluări
- Agreement To Compensation of Employee & Employer: Please Check Appropriate BoxDocument1 paginăAgreement To Compensation of Employee & Employer: Please Check Appropriate Boxc.bartleyÎncă nu există evaluări
- Compromise & Release - Pending Interpretation & Signature (Signed)Document9 paginiCompromise & Release - Pending Interpretation & Signature (Signed)Jeos DelaniÎncă nu există evaluări
- Sav 1522Document4 paginiSav 1522Michael100% (1)
- Sav 2966Document2 paginiSav 2966Michael100% (1)
- Ssa 11Document11 paginiSsa 11Carolina Bareño DuitamaÎncă nu există evaluări
- Temporary-Officiant-Application Washington DCDocument1 paginăTemporary-Officiant-Application Washington DCcboy1790Încă nu există evaluări
- BI FORM (Latest As of June 13, 2010)Document6 paginiBI FORM (Latest As of June 13, 2010)PAPARUSAÎncă nu există evaluări
- Request To Be Selected As Payee: For Ssa Use OnlyDocument10 paginiRequest To Be Selected As Payee: For Ssa Use OnlyJuanÎncă nu există evaluări
- Sav1455 PDFDocument6 paginiSav1455 PDFTed100% (1)
- Gsis Lease With Option To Buy (Lwob) : Application InformationDocument2 paginiGsis Lease With Option To Buy (Lwob) : Application InformationOlivia Abac100% (1)
- ELIB Group Claims Claimant Statement FormDocument2 paginiELIB Group Claims Claimant Statement FormPnk Telok KemangÎncă nu există evaluări
- (For Deferred Action) : G-325A, Biographic InformationDocument2 pagini(For Deferred Action) : G-325A, Biographic InformationIsrael de MelloÎncă nu există evaluări
- Dental Reimbursement 2010Document6 paginiDental Reimbursement 2010marcelo galarzaÎncă nu există evaluări
- Group Claims Claimant Statement FormDocument2 paginiGroup Claims Claimant Statement FormPnk Telok KemangÎncă nu există evaluări
- Uolus Kandidatų Anketa ENDocument3 paginiUolus Kandidatų Anketa ENABID AKHTERÎncă nu există evaluări
- Land Bank of The Philippines Livelihood Loan Application/Agreement FormDocument1 paginăLand Bank of The Philippines Livelihood Loan Application/Agreement Formjay100% (2)
- Mark Landon Financial Inc Owner Bankruptcy Filing 9/10/09 Georgia FloridaDocument70 paginiMark Landon Financial Inc Owner Bankruptcy Filing 9/10/09 Georgia FloridadocsupdateÎncă nu există evaluări
- Golden Angel Knights 2306 SecsDocument1 paginăGolden Angel Knights 2306 SecsJay-r Dela Cruz CubangbangÎncă nu există evaluări
- BR Frms Ir 83-170 1516216505344 EngDocument2 paginiBR Frms Ir 83-170 1516216505344 EngRuslan DavidenkoÎncă nu există evaluări
- 2306 Jan 2018 ENCS v4Document33 pagini2306 Jan 2018 ENCS v4nicky tampocÎncă nu există evaluări
- Affidavit of Ownership or ControlDocument3 paginiAffidavit of Ownership or ControlTexas Watchdog0% (1)
- Rep PayeeDocument12 paginiRep Payeermckane100% (1)
- Sample Chapter 13 PetitionDocument47 paginiSample Chapter 13 PetitionMaxwell Law Firm, PLLC100% (1)
- Municipal Trial Court in Cities: Bacoor City, CaviteDocument32 paginiMunicipal Trial Court in Cities: Bacoor City, Caviteモーラーリー いたちÎncă nu există evaluări
- AGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsDocument5 paginiAGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsCreations CloverÎncă nu există evaluări
- GM PetitionDocument24 paginiGM PetitionZerohedgeÎncă nu există evaluări
- BMS Virtual Claim Form Fill-In Version 0320Document1 paginăBMS Virtual Claim Form Fill-In Version 0320shane ragerÎncă nu există evaluări
- Municipal Trial Court in Cities: Bacoor City, CaviteDocument32 paginiMunicipal Trial Court in Cities: Bacoor City, Caviteモーラーリー いたちÎncă nu există evaluări
- Leslie Andre Ezidore Bankruptcy AbuseDocument17 paginiLeslie Andre Ezidore Bankruptcy AbuseKamatÎncă nu există evaluări
- Immigrant Petition by Standalone Investor: Department of Homeland Security Uscis Form I-526Document18 paginiImmigrant Petition by Standalone Investor: Department of Homeland Security Uscis Form I-526Darshan pipaliyaÎncă nu există evaluări
- Statutory Documents - CBREDocument9 paginiStatutory Documents - CBRERohit PatnalaÎncă nu există evaluări
- Sw-1621406230-Form 14b - 230710 - 094646Document4 paginiSw-1621406230-Form 14b - 230710 - 094646protaz christopherÎncă nu există evaluări
- Pagsinag RA Forms March 2022Document15 paginiPagsinag RA Forms March 2022Angelica Perlyn AurelioÎncă nu există evaluări
- TSP Withdrawl PDFDocument5 paginiTSP Withdrawl PDFMatt SmithÎncă nu există evaluări
- Fa 4126vaDocument8 paginiFa 4126vaSadia KhadimÎncă nu există evaluări
- BIRSALA Membership Form-June 2022Document1 paginăBIRSALA Membership Form-June 2022cris gerard trinidadÎncă nu există evaluări
- Certificate of Final Tax Withheld at Source: (MM/DD/YYYY) (MM/DD/YYYY)Document2 paginiCertificate of Final Tax Withheld at Source: (MM/DD/YYYY) (MM/DD/YYYY)ROGER DRIO, JRÎncă nu există evaluări
- The National Insurance Board of Trinidad and Tobago Maternity Benefit ApplicationDocument5 paginiThe National Insurance Board of Trinidad and Tobago Maternity Benefit ApplicationAriÎncă nu există evaluări
- Tan 49 BDocument3 paginiTan 49 BTanu ThakurÎncă nu există evaluări
- Form 14b EmptyDocument3 paginiForm 14b Emptypunit vinodÎncă nu există evaluări
- FLR 08A Sept105 EN FilDocument5 paginiFLR 08A Sept105 EN FilAnonymous Y2QBKwÎncă nu există evaluări
- Change of First NameDocument3 paginiChange of First NameSantos JewelÎncă nu există evaluări
- Registration Request FormDocument1 paginăRegistration Request Formalpha taurusÎncă nu există evaluări
- Application For Provident Benefits (Apb) ClaimDocument2 paginiApplication For Provident Benefits (Apb) ClaimLIERAÎncă nu există evaluări
- SBP Prescribed Application Form For Governments Profit Subsidy Facility (English)Document6 paginiSBP Prescribed Application Form For Governments Profit Subsidy Facility (English)muhammadTzÎncă nu există evaluări
- Doh 4380Document2 paginiDoh 4380Andrea Victoria Hermosilla GuedeÎncă nu există evaluări
- PAGIBIG Application For Provident Benefits ClaimDocument2 paginiPAGIBIG Application For Provident Benefits ClaimMeal StubÎncă nu există evaluări
- AX Rganizer: File Your Taxes in Just Simple Steps!Document9 paginiAX Rganizer: File Your Taxes in Just Simple Steps!Anonymous Lwhi0VzÎncă nu există evaluări
- Cory Disotell Bankruptcy FilingDocument5 paginiCory Disotell Bankruptcy FilingErin LaviolaÎncă nu există evaluări
- ABSLDocument3 paginiABSLARVINDÎncă nu există evaluări
- United States Bankruptcy Court District of Colorado Voluntary PetitionDocument49 paginiUnited States Bankruptcy Court District of Colorado Voluntary PetitionJessica McBrideÎncă nu există evaluări
- Scott Ostrem Bankruptcy DocumentDocument49 paginiScott Ostrem Bankruptcy DocumentMichael_Lee_RobertsÎncă nu există evaluări
- Individuals: Account Opening Form For F. No.-401Document17 paginiIndividuals: Account Opening Form For F. No.-401Kishor AgrawalÎncă nu există evaluări
- Fin 300 NameappDocument2 paginiFin 300 NameappDemetris NobleÎncă nu există evaluări
- SSSForm Direct House Repair PDFDocument2 paginiSSSForm Direct House Repair PDFVictor MontaÎncă nu există evaluări
- General Growth Properties' Full PetitionDocument63 paginiGeneral Growth Properties' Full PetitionDealBook100% (2)
- Application - To - Rent 2 PDFDocument3 paginiApplication - To - Rent 2 PDFDimitrios LatsisÎncă nu există evaluări
- Remedies For Breach of Contract 123Document14 paginiRemedies For Breach of Contract 123karthi100% (1)
- Directorate of Treasuries and Accounts Andhra Pradesh: Amaravati at Ibrahimpatnam FIN02-11044/22/2019-A SEC-DTA 1026331Document7 paginiDirectorate of Treasuries and Accounts Andhra Pradesh: Amaravati at Ibrahimpatnam FIN02-11044/22/2019-A SEC-DTA 1026331NAGA SATYANARAYANA NELLURIÎncă nu există evaluări
- Land Law 1Document2 paginiLand Law 1Michelle EkezieÎncă nu există evaluări
- Witness Affidavit of Emeteria B, ZuasolaDocument4 paginiWitness Affidavit of Emeteria B, ZuasolaNadin MorgadoÎncă nu există evaluări
- Chapter Vii: Due Process of Law NO. 8Document5 paginiChapter Vii: Due Process of Law NO. 8Incess CessÎncă nu există evaluări
- Berciles v. GsisDocument2 paginiBerciles v. GsisQueenie Boado100% (2)
- Resident Marine Mammals of The Protected Seascape Tañon Strait vs. ReyesDocument2 paginiResident Marine Mammals of The Protected Seascape Tañon Strait vs. ReyesElaine Honrade100% (3)
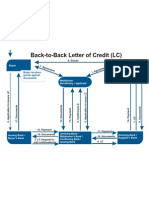
- Back To Back LCDocument1 paginăBack To Back LCJayant Nair0% (1)
- Criminal Procedure 2020Document182 paginiCriminal Procedure 2020nomsa mweetwaÎncă nu există evaluări
- The Indian Legal System An Enquiry 1St Edition Mahendra Pal Singh Download 2024 Full ChapterDocument47 paginiThe Indian Legal System An Enquiry 1St Edition Mahendra Pal Singh Download 2024 Full Chapterjames.scholtens848100% (11)
- 80 Iconic Judgments On Cheque Bounce in 2019 You Should Not Miss!Document20 pagini80 Iconic Judgments On Cheque Bounce in 2019 You Should Not Miss!naveen KumarÎncă nu există evaluări
- Consumer Protection Act, 1986Document34 paginiConsumer Protection Act, 1986dreamza2z50% (2)
- Smiley First, LLC v. Dep't of Transportation, No. SJC-13300 (Mass. May 23, 2023)Document24 paginiSmiley First, LLC v. Dep't of Transportation, No. SJC-13300 (Mass. May 23, 2023)RHTÎncă nu există evaluări
- 90 Maraguinot V NLRCDocument4 pagini90 Maraguinot V NLRCfullgrinÎncă nu există evaluări
- Petition To Approve AccountingDocument6 paginiPetition To Approve AccountingBryan Coryell100% (2)
- Immigration Consequences of Criminal Convictions in VirginiaDocument22 paginiImmigration Consequences of Criminal Convictions in VirginiaBrandon Jaycox100% (1)
- People v. Golem Sota FULL CASEDocument17 paginiPeople v. Golem Sota FULL CASEAndrei Hans Ochoa PunoÎncă nu există evaluări
- Right of Way Grant TemplateDocument5 paginiRight of Way Grant TemplateImran GhifariaÎncă nu există evaluări
- Case Comment PORTUGAL V INDIADocument3 paginiCase Comment PORTUGAL V INDIAAnshu Goel50% (2)
- Ethical Issues in Employment LawDocument5 paginiEthical Issues in Employment LawSnigdharani MajhiÎncă nu există evaluări
- J&K Services Selection Board: Applied Application Form For Appointment To Class-IvDocument3 paginiJ&K Services Selection Board: Applied Application Form For Appointment To Class-IvVijay SarmalÎncă nu există evaluări
- ConfirmationDocument5 paginiConfirmationMuni ReddyÎncă nu există evaluări
- Vinzons-Magana Vs EstrellaDocument1 paginăVinzons-Magana Vs EstrellaAthena Santos0% (1)
- Probation of Offender ActDocument6 paginiProbation of Offender ActPintu RaoÎncă nu există evaluări
- Administration of Estates Act, 1961Document46 paginiAdministration of Estates Act, 1961Maame Ekua Yaakwae AsaamÎncă nu există evaluări
- Bsa26 Cased Digestn05 de JesusDocument13 paginiBsa26 Cased Digestn05 de JesusDarid De JesusÎncă nu există evaluări
- Affidavit Solidum SharesDocument3 paginiAffidavit Solidum SharesMary.Rose RosalesÎncă nu există evaluări
- Assignment 1 BUS LAWDocument8 paginiAssignment 1 BUS LAWaliaÎncă nu există evaluări
- Arrest 6Document6 paginiArrest 6Christina StricklandÎncă nu există evaluări
- Fraud On The Court - Emergency Motion To Vacate JudgmentDocument4 paginiFraud On The Court - Emergency Motion To Vacate Judgmentwinstons231193% (27)