S-ar putea să vă placă și
- Jharkhand DV List5Document7 paginiJharkhand DV List5Ram Kumar YadavÎncă nu există evaluări
- Uttarakhand DV List5Document5 paginiUttarakhand DV List5Ram Kumar YadavÎncă nu există evaluări
- W W A L W P I U S: Omen Orkers ND Abour Elfare Rovisions N Norganised EctorDocument10 paginiW W A L W P I U S: Omen Orkers ND Abour Elfare Rovisions N Norganised EctorRam Kumar YadavÎncă nu există evaluări
- UttarPradesh DV List6Document9 paginiUttarPradesh DV List6Ram Kumar YadavÎncă nu există evaluări
- Intra Games 2022Document16 paginiIntra Games 2022Ram Kumar YadavÎncă nu există evaluări
- Odisha DV List5Document18 paginiOdisha DV List5Ram Kumar YadavÎncă nu există evaluări
- HimachalPradesh DV List5Document11 paginiHimachalPradesh DV List5Ram Kumar YadavÎncă nu există evaluări
- Modified Syllabus of Law of TaxationDocument9 paginiModified Syllabus of Law of TaxationRam Kumar YadavÎncă nu există evaluări
- Research Paper 2 Ipc DecrmininalisationDocument11 paginiResearch Paper 2 Ipc DecrmininalisationRam Kumar YadavÎncă nu există evaluări
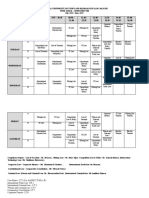
- SEM VIII Time Table-Draft-2Document2 paginiSEM VIII Time Table-Draft-2Ram Kumar YadavÎncă nu există evaluări
- The National University of Study and Research in Law, RanchiDocument2 paginiThe National University of Study and Research in Law, RanchiRam Kumar YadavÎncă nu există evaluări
- Base Price - BPL 2022Document4 paginiBase Price - BPL 2022Ram Kumar YadavÎncă nu există evaluări
- International Criminal Law Under Graduate - Viii Semester SESSION 2021-2022 (February - June)Document6 paginiInternational Criminal Law Under Graduate - Viii Semester SESSION 2021-2022 (February - June)Ram Kumar Yadav100% (1)
- NUSRL-Syllabus-Women & Criminal LawDocument3 paginiNUSRL-Syllabus-Women & Criminal LawRam Kumar YadavÎncă nu există evaluări
- Iirfrq Rtna: Central Lnstitute of PsychiatryDocument1 paginăIirfrq Rtna: Central Lnstitute of PsychiatryRam YadavÎncă nu există evaluări
- Code of Conduct NUSRL1Document4 paginiCode of Conduct NUSRL1Ram Kumar YadavÎncă nu există evaluări
- Sem I Sec BDocument6 paginiSem I Sec BRam Kumar YadavÎncă nu există evaluări
- Sem III Sec BDocument6 paginiSem III Sec BRam Kumar YadavÎncă nu există evaluări
- List of Electives - Send To Students-3rd August2021.Document2 paginiList of Electives - Send To Students-3rd August2021.Ram Kumar YadavÎncă nu există evaluări
- SEM VIII Time Table TentativeDocument2 paginiSEM VIII Time Table TentativeRam Kumar YadavÎncă nu există evaluări
- PG Semester IDocument15 paginiPG Semester IRam Kumar YadavÎncă nu există evaluări
- Information Bulletin: Ctet - DecemberDocument56 paginiInformation Bulletin: Ctet - Decembershubham anandÎncă nu există evaluări
- Law of Adr & Arbitration: Submitted To Submitted byDocument16 paginiLaw of Adr & Arbitration: Submitted To Submitted byRam Kumar YadavÎncă nu există evaluări
- List of Electives in Semester VIIDocument1 paginăList of Electives in Semester VIIRam Kumar YadavÎncă nu există evaluări
- BPSC 67th Combined Competitive Exam 2021: 555 Posts Apply From Sept 30Document9 paginiBPSC 67th Combined Competitive Exam 2021: 555 Posts Apply From Sept 30Rajesh K KumarÎncă nu există evaluări
- Sem VII Time TableDocument1 paginăSem VII Time TableRam YadavÎncă nu există evaluări
- Semester III Section A - Final ResultDocument6 paginiSemester III Section A - Final ResultRam Kumar YadavÎncă nu există evaluări
- C N L U: Hanakya Ational AW NiversityDocument18 paginiC N L U: Hanakya Ational AW NiversityMukesh TomarÎncă nu există evaluări
- National University of Study and Research in Law, Ranchi Final Result Family Law II (Code: L 108) Semester IV B.A. LL.B. (Hons.), Batch 2019 (Section A)Document6 paginiNational University of Study and Research in Law, Ranchi Final Result Family Law II (Code: L 108) Semester IV B.A. LL.B. (Hons.), Batch 2019 (Section A)Ram YadavÎncă nu există evaluări
- Ipr-Ii Research PaperDocument18 paginiIpr-Ii Research PaperRam Kumar YadavÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Gynocology Formulas: Summary: Gu Yin Jian Shou Tai Wan An Tai Yin Nei Bu WanDocument4 paginiGynocology Formulas: Summary: Gu Yin Jian Shou Tai Wan An Tai Yin Nei Bu WanYumbalum100% (1)
- Purdon, Christine - Clark, David A - Overcoming Obsessive Thoughts - How To Gain Control of Your OCD (2005, New Harbinger Publications)Document175 paginiPurdon, Christine - Clark, David A - Overcoming Obsessive Thoughts - How To Gain Control of Your OCD (2005, New Harbinger Publications)fercin180% (5)
- The 7-Day Happiness Challenge - The New York TimesDocument5 paginiThe 7-Day Happiness Challenge - The New York TimesIvan MoreiraÎncă nu există evaluări
- Perdev Reader Activity 1Document23 paginiPerdev Reader Activity 1Gin LaguitaoÎncă nu există evaluări
- Neurological Examination - Pre-Med - 401Document73 paginiNeurological Examination - Pre-Med - 401Surat Tanprawate100% (4)
- Motivation 9-10Document74 paginiMotivation 9-10krishnasree100% (1)
- Undifferentiated Schizophrenia Case AnalysisDocument17 paginiUndifferentiated Schizophrenia Case Analysisaaron tabernaÎncă nu există evaluări
- M.K.M. LunnemannDocument12 paginiM.K.M. Lunnemannale_isa_naÎncă nu există evaluări
- A Conceptual Framework For Developing and Evaluating Behavior Change Interventions For Injury ControlDocument13 paginiA Conceptual Framework For Developing and Evaluating Behavior Change Interventions For Injury ControlErik SaucedoÎncă nu există evaluări
- Innovative Use of Virtual Reality in Autism Spectrum Disorder: A Case-StudyDocument12 paginiInnovative Use of Virtual Reality in Autism Spectrum Disorder: A Case-StudyomenpkuÎncă nu există evaluări
- Textbook of EndodonticsDocument602 paginiTextbook of EndodonticsThin Tranphuoc100% (2)
- QR Scientifique Technique EN 011119Document29 paginiQR Scientifique Technique EN 011119Vio CondreiÎncă nu există evaluări
- 24 Periop Hemodynamic Instability, Consensus, APSFDocument12 pagini24 Periop Hemodynamic Instability, Consensus, APSFabsenrifkyjamalÎncă nu există evaluări
- Medicin Der Virker: Martin S. Knudsen Senior Consultant IMS Health Economics and Outcomes ResearchDocument16 paginiMedicin Der Virker: Martin S. Knudsen Senior Consultant IMS Health Economics and Outcomes ResearchdagensmedicinÎncă nu există evaluări
- Presentation - Aging 2.0 San Diego Nov 05,19Document26 paginiPresentation - Aging 2.0 San Diego Nov 05,19Bijou LullaÎncă nu există evaluări
- ENG 111-054 - Legalized Euthanasia As Opposed To HospiceDocument5 paginiENG 111-054 - Legalized Euthanasia As Opposed To HospiceBee ThaoÎncă nu există evaluări
- Aesthetic Inlays: November 2011Document4 paginiAesthetic Inlays: November 2011Diego SarunÎncă nu există evaluări
- LSI Brgy. CertificationDocument2 paginiLSI Brgy. CertificationRuth BolongaitaÎncă nu există evaluări
- Yua Mikami 三上悠亜Document5 paginiYua Mikami 三上悠亜Devon DudleyÎncă nu există evaluări
- Group4 A6-1Document84 paginiGroup4 A6-1JulietteÎncă nu există evaluări
- LĐ - Reading Full Test 1 - HsDocument8 paginiLĐ - Reading Full Test 1 - HsNguyen Vu Thuy DuongÎncă nu există evaluări
- Human Resource ManagementDocument18 paginiHuman Resource ManagementT S Kumar KumarÎncă nu există evaluări
- Chakras Chart PDFDocument1 paginăChakras Chart PDFTushar Sapkal100% (2)
- 3 Year Plan Badac Action PlanDocument2 pagini3 Year Plan Badac Action PlanJean LebiosÎncă nu există evaluări
- Jurnal No 3 (Learning Cycle 5E)Document7 paginiJurnal No 3 (Learning Cycle 5E)Alma SiwiÎncă nu există evaluări
- Interventions For Preventing Falls in People After Stroke (Review)Document68 paginiInterventions For Preventing Falls in People After Stroke (Review)Abdelrhman AhmedÎncă nu există evaluări
- 166-176 The Role of Financial Behavior in Mediation The Influence of Financial Literacy and Financial Self Efficacy On Financial Will BeingDocument11 pagini166-176 The Role of Financial Behavior in Mediation The Influence of Financial Literacy and Financial Self Efficacy On Financial Will BeingJuvy ParaguyaÎncă nu există evaluări
- TELEMEDICINEDocument2 paginiTELEMEDICINESILLA ELSA SOJIÎncă nu există evaluări
- Sudha - : Learning and Development at 3MDocument3 paginiSudha - : Learning and Development at 3MVardhan BhosaleÎncă nu există evaluări
- DAFTARRUJUKANDocument4 paginiDAFTARRUJUKANIndahÎncă nu există evaluări