S-ar putea să vă placă și
- Running Head: Critical Analysis ReportDocument8 paginiRunning Head: Critical Analysis Reportapi-277510691Încă nu există evaluări
- Medical Necessity Guidelines: Behavioral Health Evidence-Based Practices (EBP)Document5 paginiMedical Necessity Guidelines: Behavioral Health Evidence-Based Practices (EBP)Carol Golden GuidryÎncă nu există evaluări
- Home VisitDocument2 paginiHome VisitPrincess Gwyneth MartinezÎncă nu există evaluări
- Family Health 2Document42 paginiFamily Health 2coosa liquorsÎncă nu există evaluări
- Home VisitDocument17 paginiHome VisitKrystel Joy AuroÎncă nu există evaluări
- ABA Service AgreementDocument3 paginiABA Service AgreementEva BrownÎncă nu există evaluări
- Talking Points 05092005Document10 paginiTalking Points 05092005profanejustice100% (1)
- RN Home Health Primary 800013 Home HealthDocument5 paginiRN Home Health Primary 800013 Home Healthدكتور محمد بايونييرÎncă nu există evaluări
- Home VisitDocument17 paginiHome VisitMamta Rajput100% (2)
- CHN - Written ReportDocument3 paginiCHN - Written ReportJastine DiazÎncă nu există evaluări
- Page 1 of 4Document4 paginiPage 1 of 4UWTSSÎncă nu există evaluări
- Team Cerulean BlackDocument18 paginiTeam Cerulean BlackEmmanuel AbiolaÎncă nu există evaluări
- Swbest Practices PDFDocument6 paginiSwbest Practices PDFMary Grace Dionisio-RodriguezÎncă nu există evaluări
- Famcare 04Document26 paginiFamcare 04droulaki1991Încă nu există evaluări
- PDF DocumentDocument36 paginiPDF DocumentSuji MerlineÎncă nu există evaluări
- 10.10 Comprehensive Child and Family Assessment (CCFA)Document8 pagini10.10 Comprehensive Child and Family Assessment (CCFA)shemariyahsworldÎncă nu există evaluări
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsDe la EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsÎncă nu există evaluări
- TN BH ABA Provider OrientationDocument34 paginiTN BH ABA Provider OrientationVivian ChenÎncă nu există evaluări
- What Is California's Continuum of Care ReformDocument2 paginiWhat Is California's Continuum of Care ReformKQED NewsÎncă nu există evaluări
- Chief Psychiatrist Discharge Planning PDFDocument8 paginiChief Psychiatrist Discharge Planning PDFMaddy HuckelÎncă nu există evaluări
- Interact Treatment Manual & Participant Workbook: Based on the Self Help Theory of Jim MaclaineDe la EverandInteract Treatment Manual & Participant Workbook: Based on the Self Help Theory of Jim MaclaineÎncă nu există evaluări
- PDF GettingStarted-AmbulatoryCareDocument27 paginiPDF GettingStarted-AmbulatoryCareChristian SoberonÎncă nu există evaluări
- Brunswick County Considers Using Opioid Settlement Funding For Substance Abuse ClinicianDocument3 paginiBrunswick County Considers Using Opioid Settlement Funding For Substance Abuse ClinicianJamie BouletÎncă nu există evaluări
- Framework For Ethical Decision-Making: Answer The Following Questions in Your Group. in Each of TheDocument4 paginiFramework For Ethical Decision-Making: Answer The Following Questions in Your Group. in Each of Theapi-309879220Încă nu există evaluări
- Family Health ManagementDocument12 paginiFamily Health ManagementVincent CuyucaÎncă nu există evaluări
- Job Spec HSE Area Lead of Service User Family CarerDocument7 paginiJob Spec HSE Area Lead of Service User Family CarerGateway ProjectÎncă nu există evaluări
- Progress Note Training (TCM)Document39 paginiProgress Note Training (TCM)jv10gmailÎncă nu există evaluări
- Treating Adolescent Substance Abuse Using Family Behavior Therapy: A Step-by-Step ApproachDe la EverandTreating Adolescent Substance Abuse Using Family Behavior Therapy: A Step-by-Step ApproachÎncă nu există evaluări
- Community Health Nursing ManualDocument23 paginiCommunity Health Nursing ManualNurjanna AdjilulÎncă nu există evaluări
- Non Compliance NCPDocument3 paginiNon Compliance NCPlibdub75% (4)
- The Numbered LetterDocument13 paginiThe Numbered LetterChildren's Hospice & Palliative Care CoalitionÎncă nu există evaluări
- Community Treatment Orders Treatment Plan GuidelinesDocument4 paginiCommunity Treatment Orders Treatment Plan GuidelinesrelalisaramaÎncă nu există evaluări
- Home VisitDocument6 paginiHome VisitRaida Marañon Ibrahim60% (5)
- Presentor-: Ruma Sen: MN (Previous) RakconDocument40 paginiPresentor-: Ruma Sen: MN (Previous) Rakconcy100% (1)
- 2107 - Intro Family PreservationDocument5 pagini2107 - Intro Family PreservationshemariyahsworldÎncă nu există evaluări
- Family Health Nursing Care ProcessDocument2 paginiFamily Health Nursing Care ProcessAnnalisa TellesÎncă nu există evaluări
- J Promoting Health and Wellness PolicyDocument11 paginiJ Promoting Health and Wellness PolicyRick ThomaÎncă nu există evaluări
- POLICYDocument6 paginiPOLICYBijula ManjuÎncă nu există evaluări
- PALMAR Answer KeysDocument64 paginiPALMAR Answer KeysDanica SaronÎncă nu există evaluări
- Records in Family Health Nursing PracticeDocument6 paginiRecords in Family Health Nursing PracticeA.j. Caraca89% (9)
- Mental Health Treatment Plans North Western Melbourne PHNDocument14 paginiMental Health Treatment Plans North Western Melbourne PHNMeryel de los Santos100% (2)
- Unit 4222-328Document6 paginiUnit 4222-328Akular Ayram100% (1)
- Physiotherapy AssistantDocument10 paginiPhysiotherapy AssistantOscar NgÎncă nu există evaluări
- BT 2022107Document3 paginiBT 2022107Indiana Family to FamilyÎncă nu există evaluări
- Behavioral Health Director August 2011Document3 paginiBehavioral Health Director August 2011NASWCAÎncă nu există evaluări
- ASI Treatment Planning ManualDocument22 paginiASI Treatment Planning Manualdrmss100% (1)
- Ethical, Legal, and Economic Foundations of The Educational Process - BUGHAO, MARIA ANGELIKADocument4 paginiEthical, Legal, and Economic Foundations of The Educational Process - BUGHAO, MARIA ANGELIKAMaria Angelika BughaoÎncă nu există evaluări
- Home VisitDocument15 paginiHome VisitAnthony Andrei IzonÎncă nu există evaluări
- C. Formulating Family Nursing Care PlanDocument35 paginiC. Formulating Family Nursing Care PlanWilma BeraldeÎncă nu există evaluări
- Community Health Nursing ProcessDocument35 paginiCommunity Health Nursing Processdave100% (1)
- Home Care LEARNING OUTCOMES After Completing This Chapter, YouDocument18 paginiHome Care LEARNING OUTCOMES After Completing This Chapter, Youtwy113100% (1)
- Standard Health CareDocument3 paginiStandard Health Careجنان منيرÎncă nu există evaluări
- Home VisitDocument9 paginiHome VisitHydra Olivar - Pantilgan100% (2)
- Home VisitDocument9 paginiHome VisitHydra Olivar - PantilganÎncă nu există evaluări
- Consultant PsychiatristDocument13 paginiConsultant PsychiatristDaniel LuuÎncă nu există evaluări
- The Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansDe la EverandThe Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansÎncă nu există evaluări
- Improved Family Friendly Measures PDFDocument37 paginiImproved Family Friendly Measures PDFgtecmaltaÎncă nu există evaluări
- Lac ProceduresDocument34 paginiLac ProceduresGinaAlexaCîmpianuÎncă nu există evaluări
- Memorandum of Understanding Between Child Welfare / Community Service Providers - Florida - (2004) .Document12 paginiMemorandum of Understanding Between Child Welfare / Community Service Providers - Florida - (2004) .Rick ThomaÎncă nu există evaluări
- Brain Nutrients PDFDocument10 paginiBrain Nutrients PDFBj LongÎncă nu există evaluări
- Garner 1511222Document17 paginiGarner 1511222Bj LongÎncă nu există evaluări
- Life Skills Coach OverviewDocument1 paginăLife Skills Coach OverviewBj LongÎncă nu există evaluări
- Good Kids With Bad Behaviors: Life Skills CoachingDocument3 paginiGood Kids With Bad Behaviors: Life Skills CoachingBj LongÎncă nu există evaluări
- A Palace in Time ReviewDocument6 paginiA Palace in Time ReviewBj LongÎncă nu există evaluări
- Court of Claims Argued in 06Document416 paginiCourt of Claims Argued in 06Bj LongÎncă nu există evaluări
- HealingToothDecay PDFDocument6 paginiHealingToothDecay PDFBj Long100% (1)
- The Morning Meditation Long FormDocument46 paginiThe Morning Meditation Long FormBj LongÎncă nu există evaluări
- AA WivesDocument4 paginiAA WivesBj Long100% (2)
- A Two-Way Prayer: Answer Me When I Call To You, O My Righteous God. (Psalm 4:1a, NIV)Document2 paginiA Two-Way Prayer: Answer Me When I Call To You, O My Righteous God. (Psalm 4:1a, NIV)Bj LongÎncă nu există evaluări
- Bảo MậtDocument2 paginiBảo MậtMinh Nghia PhamÎncă nu există evaluări
- Remedial Law Syllabus 2013Document6 paginiRemedial Law Syllabus 2013Mirriam Ebreo100% (1)
- Unit 4 Pharmacognsosy 2 - 5th SemDocument16 paginiUnit 4 Pharmacognsosy 2 - 5th SemJagadeeshkeerthi KeerthiÎncă nu există evaluări
- Sustainability and Economy - A Paradigm For Managing Entrepreneurship Towards Sustainable DevelopmentFDocument21 paginiSustainability and Economy - A Paradigm For Managing Entrepreneurship Towards Sustainable DevelopmentFArmando Tarupí MontenegroÎncă nu există evaluări
- DTR For ReadingDocument2 paginiDTR For ReadingTimosa TeyobÎncă nu există evaluări
- Santa Letters 2013Document16 paginiSanta Letters 2013Lebanon_PublishingÎncă nu există evaluări
- Chapter 9 CompensationDocument24 paginiChapter 9 CompensationSophie CheungÎncă nu există evaluări
- Adaptation Fom Squirrels GamesDocument2 paginiAdaptation Fom Squirrels GamesDenny Boy MochranÎncă nu există evaluări
- Definition of Unit HydrographDocument5 paginiDefinition of Unit HydrographPankaj ChowdhuryÎncă nu există evaluări
- Management Thoughts Pramod Batra PDFDocument5 paginiManagement Thoughts Pramod Batra PDFRam33% (3)
- WabimalunoxowevefoDocument3 paginiWabimalunoxowevefoChitmin KhantÎncă nu există evaluări
- FIN323 Project 2021-2022Document6 paginiFIN323 Project 2021-2022saleem razaÎncă nu există evaluări
- 3rd Term s1 Agricultural Science 1Document41 pagini3rd Term s1 Agricultural Science 1Adelowo DanielÎncă nu există evaluări
- Vol 17 No 3 and No 4 Fort Laramie and The Sioux War of 1876Document19 paginiVol 17 No 3 and No 4 Fort Laramie and The Sioux War of 1876Лазар СрећковићÎncă nu există evaluări
- Ranbaxy Acquisition by DaiichiDocument9 paginiRanbaxy Acquisition by Daiichirupe59Încă nu există evaluări
- Lean ManufacturingDocument61 paginiLean ManufacturingWasiYamanChoudhuryÎncă nu există evaluări
- HCL Corporate-PresentationDocument14 paginiHCL Corporate-Presentationtony_reddyÎncă nu există evaluări
- PDF of Proposed Museum ProjectDocument145 paginiPDF of Proposed Museum ProjectHarshita ParnamiÎncă nu există evaluări
- 24th SFCON Parallel Sessions Schedule (For Souvenir Program)Document1 pagină24th SFCON Parallel Sessions Schedule (For Souvenir Program)genesistorres286Încă nu există evaluări
- A Laboratory Study of Hot Carbon Dioxide Injection Into Fractured and Conventional CoresDocument13 paginiA Laboratory Study of Hot Carbon Dioxide Injection Into Fractured and Conventional Coresmsmsoft90Încă nu există evaluări
- Teit Cbgs Dmbi Lab Manual FH 2015Document60 paginiTeit Cbgs Dmbi Lab Manual FH 2015Soumya PandeyÎncă nu există evaluări
- Westermo MRD 330-3xx & GreenBow IPSec VPN Client Software ConfigurationDocument12 paginiWestermo MRD 330-3xx & GreenBow IPSec VPN Client Software ConfigurationgreenbowÎncă nu există evaluări
- The Cycle of Leadership Through Transformational, Eccles - (Leadership) PDFDocument16 paginiThe Cycle of Leadership Through Transformational, Eccles - (Leadership) PDFEliana LopezÎncă nu există evaluări
- Flexi Multiradio Introduction - Sharing SessionDocument96 paginiFlexi Multiradio Introduction - Sharing SessionRobby MiloÎncă nu există evaluări
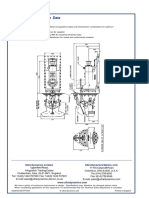
- Ultrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedDocument2 paginiUltrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedhaujesÎncă nu există evaluări
- API Design GiudeDocument9 paginiAPI Design GiudeTamilarasi DhanakodiÎncă nu există evaluări
- SamanthavasquezresumeDocument1 paginăSamanthavasquezresumeapi-278808369Încă nu există evaluări
- Bharati AXA Life InsuranceDocument57 paginiBharati AXA Life InsuranceNaina_Dwivedi_6514100% (3)
- CM760 E-Brochure HemobasculaDocument6 paginiCM760 E-Brochure Hemobasculajordigs50Încă nu există evaluări
- IMO - PowerpointDocument16 paginiIMO - PowerpointMahen Fernando100% (3)