S-ar putea să vă placă și
- La Union Arrival Card - V1 PDFDocument2 paginiLa Union Arrival Card - V1 PDFLorei Lee100% (1)
- La Union Arrival Card - V1 PDFDocument2 paginiLa Union Arrival Card - V1 PDFChachi SorianoÎncă nu există evaluări
- La Union Arrival Card - V1 PDFDocument2 paginiLa Union Arrival Card - V1 PDFAdrian DoctoleroÎncă nu există evaluări
- La Union Arrival Card V1Document2 paginiLa Union Arrival Card V1Jovelyn MaskitÎncă nu există evaluări
- FRSC Registration Form 2Document1 paginăFRSC Registration Form 2api-315742494Încă nu există evaluări
- Barangay Protection OrderDocument1 paginăBarangay Protection OrderJhon Lloyd Sumabat CarbonquilloÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersSarahSshiÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersJohn Joshua MontañezÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersErykah KhangÎncă nu există evaluări
- Application For Barangay Protection Order: Vawc Form#3 CONTROL NO.Document1 paginăApplication For Barangay Protection Order: Vawc Form#3 CONTROL NO.Jacjac Famador86% (7)
- Bpo Application Form: Republic of The Philippines Province of Pangasinan Municipality of Bautista Barangay SinabaanDocument1 paginăBpo Application Form: Republic of The Philippines Province of Pangasinan Municipality of Bautista Barangay SinabaanOmar Dizon II50% (2)
- Vawc Form #3 Application For BPODocument1 paginăVawc Form #3 Application For BPOJoy Toledo EnarsicoÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersMary Catherine FloraÎncă nu există evaluări
- Neppassport PDFDocument2 paginiNeppassport PDFMaria Fe Hechanova AntoloÎncă nu există evaluări
- Annex A. Application Form Final 01312022Document4 paginiAnnex A. Application Form Final 01312022Neil ryan VillarealÎncă nu există evaluări
- Incident Form For Offenses Against PersonsDocument1 paginăIncident Form For Offenses Against PersonsJanna CRIZETTEÎncă nu există evaluări
- Denr Application For Agricultural Free PatentDocument3 paginiDenr Application For Agricultural Free PatentAngelica DulceÎncă nu există evaluări
- Release Form 1Document2 paginiRelease Form 1thegrind2011Încă nu există evaluări
- DFA FormDocument2 paginiDFA FormMark Anthony Capito AñosÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersDominic MendozaÎncă nu există evaluări
- Intake Sheet For VAWCDocument2 paginiIntake Sheet For VAWCDaisy Palero Tibayan88% (8)
- Important RemindersDocument2 paginiImportant RemindersRey Razel CaveÎncă nu există evaluări
- Parents Permit 1Document1 paginăParents Permit 1Romer Ysidore SapaÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersJayson R. CabanillaÎncă nu există evaluări
- VAW Intake Form 2023Document4 paginiVAW Intake Form 2023Arnold GuintoÎncă nu există evaluări
- App FormDocument1 paginăApp FormMelchor SambranoÎncă nu există evaluări
- DaisyDocument2 paginiDaisyG-yan Dungan MamuyacÎncă nu există evaluări
- Incident Report TemplateDocument2 paginiIncident Report TemplateMostafa AbdullahÎncă nu există evaluări
- 00062018031900958Document2 pagini00062018031900958Pamela BachichaÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersAldrin Palma AyalinÎncă nu există evaluări
- RX Incident Report FormDocument2 paginiRX Incident Report FormArthur KrichevskyÎncă nu există evaluări
- Fire Incident ReportDocument2 paginiFire Incident ReportTN SanjayÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant Remindersaces solutionsÎncă nu există evaluări
- Patient Incident ReportDocument2 paginiPatient Incident ReportTN SanjayÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant Remindersroldan figuracionÎncă nu există evaluări
- Important RemindersDocument4 paginiImportant RemindersasdasdsadÎncă nu există evaluări
- Divorce Intake SheetDocument6 paginiDivorce Intake SheetJoseph Malelang100% (1)
- Vehicle Incident ReportDocument2 paginiVehicle Incident ReportTN SanjayÎncă nu există evaluări
- Public Information Request Form 1-15Document1 paginăPublic Information Request Form 1-15Diana SaffersbyÎncă nu există evaluări
- PDFDocument6 paginiPDFVincent Salarda BaldomeroÎncă nu există evaluări
- Workplace Incident ReportDocument2 paginiWorkplace Incident ReportMyo LwinÎncă nu există evaluări
- Around The Clock Childcare LTD Enrollment Form-12rieDocument4 paginiAround The Clock Childcare LTD Enrollment Form-12rieapi-251659956Încă nu există evaluări
- Important RemindersDocument2 paginiImportant Remindersrolan ambrocioÎncă nu există evaluări
- Municipal Form 103Document2 paginiMunicipal Form 103clandestine268471% (14)
- DFA Application FormDocument1 paginăDFA Application Formroadshow2381% (21)
- KHP, LLC ApplicationDocument4 paginiKHP, LLC ApplicationKeeton HanksÎncă nu există evaluări
- Sinclair Consent FormDocument1 paginăSinclair Consent Formapi-349745767Încă nu există evaluări
- Security Guard Incident ReportDocument2 paginiSecurity Guard Incident ReportArchiedm WehjrÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant Remindersasdfjkl asddfÎncă nu există evaluări
- 00152018081800020 (1)Document2 pagini00152018081800020 (1)wennielyn yuagÎncă nu există evaluări
- Vaw Form CompleteDocument7 paginiVaw Form CompleteBarangaydolores Sanpablocity75% (12)
- Important RemindersDocument2 paginiImportant RemindersHilds Osal LutoÎncă nu există evaluări
- Male Head of HouseholdDocument3 paginiMale Head of HouseholdAlexander Haruna SaturdayÎncă nu există evaluări
- Healthcare Associate Employment Application: Personal InformationDocument20 paginiHealthcare Associate Employment Application: Personal InformationShujaRehmanÎncă nu există evaluări
- Important RemindersDocument2 paginiImportant RemindersArvin PaltepÎncă nu există evaluări
- Progressive Health Care: Critical Health Care InformationDe la EverandProgressive Health Care: Critical Health Care InformationÎncă nu există evaluări
- Buble Cpap DataDocument1 paginăBuble Cpap DataTubagus JulianÎncă nu există evaluări
- Overview of Systematic Reviews of Advance Care Planning: Summary of Evidence and Global LessonsDocument49 paginiOverview of Systematic Reviews of Advance Care Planning: Summary of Evidence and Global LessonsRahmanu ReztaputraÎncă nu există evaluări
- Revised Plan For Ahsas Kafalat Progrmme District Health Authority BahawlapurDocument2 paginiRevised Plan For Ahsas Kafalat Progrmme District Health Authority BahawlapurMuhammad Shahid IqbalÎncă nu există evaluări
- Bacteriologie TI MCCDocument20 paginiBacteriologie TI MCCMihaela DomencoÎncă nu există evaluări
- Osce AbdomenDocument33 paginiOsce AbdomenistiÎncă nu există evaluări
- Maklumat Vaksinasi: Vaccination DetailsDocument1 paginăMaklumat Vaksinasi: Vaccination DetailsNURIN IRDINA BINTI AHMAD IZHAM MoeÎncă nu există evaluări
- New Instructor Application: MEDIC FIRST AID International, IncDocument2 paginiNew Instructor Application: MEDIC FIRST AID International, IncjhoniÎncă nu există evaluări
- COVID UndertakingDocument2 paginiCOVID UndertakingVickyÎncă nu există evaluări
- Five Wishes SampleDocument12 paginiFive Wishes SampleOsemeÎncă nu există evaluări
- Test Bank For Ebersole and Hess Gerontological Nursing and Healthy Aging 1st Canadian Edition TouhyDocument7 paginiTest Bank For Ebersole and Hess Gerontological Nursing and Healthy Aging 1st Canadian Edition TouhyGraceLopezyfmox100% (36)
- Microscopy Gram-Color: Stain Set For The Gram Staining MethodDocument3 paginiMicroscopy Gram-Color: Stain Set For The Gram Staining MethodMuhammad AdhityaÎncă nu există evaluări
- ახალშობილის მოვლაDocument28 paginiახალშობილის მოვლაNino KochuashviliÎncă nu există evaluări
- 158-Article Text-220-1-10-20181218Document4 pagini158-Article Text-220-1-10-20181218Fania Aulia RahmaÎncă nu există evaluări
- Bloodlines, Tubing Systems, Accessories: Product RangeDocument16 paginiBloodlines, Tubing Systems, Accessories: Product RangeEta Truta0% (1)
- CRCC11 - Leave Application Form 220309Document1 paginăCRCC11 - Leave Application Form 220309Ali md YounusÎncă nu există evaluări
- Introducing The Leadership in Enabling Occupation (LEO) ModelDocument6 paginiIntroducing The Leadership in Enabling Occupation (LEO) ModelPatricia Jara Reyes100% (1)
- Nurs FPX 4030 Assessment 2 Determining The Credibility of Evidence and ResourcesDocument5 paginiNurs FPX 4030 Assessment 2 Determining The Credibility of Evidence and Resourcesfarwaamjad771Încă nu există evaluări
- Posterior Palatal SealDocument20 paginiPosterior Palatal Seala,sajsdoqjsÎncă nu există evaluări
- Request Letter First Aid Training and BLSDocument4 paginiRequest Letter First Aid Training and BLSAlbert Dominguez100% (1)
- RG Stone Urology and Laparoscopy Hospital: SL - No. Service Particulars Units Amount (RS.)Document1 paginăRG Stone Urology and Laparoscopy Hospital: SL - No. Service Particulars Units Amount (RS.)Krishna ThakkerÎncă nu există evaluări
- StudiKualitatifImplementasiKebijakanEliminasiMalaria ASP Juni2021Document15 paginiStudiKualitatifImplementasiKebijakanEliminasiMalaria ASP Juni2021Claudya Putri AzenyÎncă nu există evaluări
- Performance Report For The Month of March 2019Document6 paginiPerformance Report For The Month of March 2019melvin terrazolaÎncă nu există evaluări
- Job Application FormDocument3 paginiJob Application Formnrynaybae.iiÎncă nu există evaluări
- Format Pendokumentasian Asuhan Kebidanan Kehamilan (Anc)Document10 paginiFormat Pendokumentasian Asuhan Kebidanan Kehamilan (Anc)Ratna DewiÎncă nu există evaluări
- The Sun 03042023Document24 paginiThe Sun 03042023Huong Zhi SanÎncă nu există evaluări
- 940837-000001 LMA-Protector Factsheet 1604Document2 pagini940837-000001 LMA-Protector Factsheet 1604nanang criztaÎncă nu există evaluări
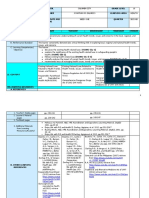
- Q2 Grade 10 HEALTH DLL Week 1Document14 paginiQ2 Grade 10 HEALTH DLL Week 1Keren Gay VillalunaÎncă nu există evaluări
- English For Nursing Topic 9 General AssessmentDocument5 paginiEnglish For Nursing Topic 9 General AssessmentMarisa Nur LailaÎncă nu există evaluări
- RTI Swasthya BhavanDocument55 paginiRTI Swasthya BhavanPrabir Kumar ChatterjeeÎncă nu există evaluări
- Primary Care (PC) and Primary Health Care (PHC) : What Is The Difference?Document3 paginiPrimary Care (PC) and Primary Health Care (PHC) : What Is The Difference?keshyaÎncă nu există evaluări