S-ar putea să vă placă și
- Final Individual Research Paper Health 101 Sec 001 Article 2Document10 paginiFinal Individual Research Paper Health 101 Sec 001 Article 2api-622203747Încă nu există evaluări
- Plos 1 - Artifact 1Document14 paginiPlos 1 - Artifact 1api-683001786Încă nu există evaluări
- Hi 225 FinalpaperDocument11 paginiHi 225 Finalpaperapi-708689221Încă nu există evaluări
- Health 101 Research PaperDocument14 paginiHealth 101 Research Paperapi-302787939Încă nu există evaluări
- HealthcareDocument6 paginiHealthcareJohnÎncă nu există evaluări
- medical english作業 PDFDocument10 paginimedical english作業 PDFeric483460Încă nu există evaluări
- Is Healthcare A Right or A PrivilegeDocument6 paginiIs Healthcare A Right or A Privilegearies usamaÎncă nu există evaluări
- HLTH 101 PaperDocument8 paginiHLTH 101 Paperapi-548493910Încă nu există evaluări
- HLTH 101 Research PaperDocument9 paginiHLTH 101 Research Paperapi-625678417Încă nu există evaluări
- 15 Finkelstein Et Al 2012 Oregon Insurance ExperimentDocument50 pagini15 Finkelstein Et Al 2012 Oregon Insurance ExperimentprithvijitmÎncă nu există evaluări
- Doctors, Hospitals, Insurers, Oh My! What You Need to know about Health Insurance and Health CareDe la EverandDoctors, Hospitals, Insurers, Oh My! What You Need to know about Health Insurance and Health CareÎncă nu există evaluări
- Health Care Schemes Project at KamineniDocument78 paginiHealth Care Schemes Project at KamineniVenugopal VutukuruÎncă nu există evaluări
- Compare and Contrast The US and KSA Health Care SystemsDocument7 paginiCompare and Contrast The US and KSA Health Care SystemsJohn NdambukiÎncă nu există evaluări
- Running Head: The Future of U.S. Healthcare System 1Document9 paginiRunning Head: The Future of U.S. Healthcare System 1Chemiati KhisaÎncă nu există evaluări
- Subsyems Policies in USADocument13 paginiSubsyems Policies in USAWanjikuÎncă nu există evaluări
- StubbertJ N362 Forum1Document4 paginiStubbertJ N362 Forum1Jane StubbertÎncă nu există evaluări
- Human Resources Within HealthcareDocument4 paginiHuman Resources Within HealthcareEdwin KimosopÎncă nu există evaluări
- Ethical Case Analysis PaperDocument14 paginiEthical Case Analysis Paperapi-282129457100% (1)
- Vero Health SystemDocument11 paginiVero Health Systemzaks mainaÎncă nu există evaluări
- Australian & Russia Healthcare System Term PaperDocument9 paginiAustralian & Russia Healthcare System Term Paperعهود الشهريÎncă nu există evaluări
- Healthcare Usa Vs Uk 12-2-18Document13 paginiHealthcare Usa Vs Uk 12-2-18api-547267182Încă nu există evaluări
- Universal Health Care Research PaperDocument5 paginiUniversal Health Care Research Paperwftvsutlg100% (1)
- HLTH 101 Final Research Paper - Due 11 30Document7 paginiHLTH 101 Final Research Paper - Due 11 30api-625713699Încă nu există evaluări
- Annotated Essay FixedDocument4 paginiAnnotated Essay Fixedapi-740539255Încă nu există evaluări
- Nu710 w5 - Paper International Healthcare SystemsDocument11 paginiNu710 w5 - Paper International Healthcare Systemsapi-577441503Încă nu există evaluări
- MBA - Pharma Healthcare Que-AnsDocument56 paginiMBA - Pharma Healthcare Que-AnskeyurÎncă nu există evaluări
- The Argumentative Essay: Health Care in AmericaDocument10 paginiThe Argumentative Essay: Health Care in AmericaRosana Cook-PowellÎncă nu există evaluări
- Revised Transcript 11 (1) .EditedDocument8 paginiRevised Transcript 11 (1) .EditedElizabeth GithinjiÎncă nu există evaluări
- The Case For Universal HealthcareDocument8 paginiThe Case For Universal HealthcareLawrence LeeÎncă nu există evaluări
- Task 3 Comparison of Health CareDocument4 paginiTask 3 Comparison of Health CareHogan ObiÎncă nu există evaluări
- Niles Chp1 2021Document22 paginiNiles Chp1 2021Trent HardestyÎncă nu există evaluări
- Title: An Essay On The Health Care Funding Structure of Australia and MexicoDocument8 paginiTitle: An Essay On The Health Care Funding Structure of Australia and MexicoSaheli Mandal MitraÎncă nu există evaluări
- Walker Style DraftDocument11 paginiWalker Style Draftapi-437845987Încă nu există evaluări
- Policy Paper DR KeysDocument12 paginiPolicy Paper DR Keysapi-295772134Încă nu există evaluări
- Econ 149 US Healthcare System vs. UK Healthcare SystemDocument5 paginiEcon 149 US Healthcare System vs. UK Healthcare SystemManu NgetichÎncă nu există evaluări
- Final Research Paper HLTH 101 3Document8 paginiFinal Research Paper HLTH 101 3api-550346996Încă nu există evaluări
- Table of Contents:: 1. Evolution of The U.S. Health Care PolicyDocument8 paginiTable of Contents:: 1. Evolution of The U.S. Health Care Policyadam tcacencoÎncă nu există evaluări
- Crisis of Abundance: Rethinking How We Pay for Health CareDe la EverandCrisis of Abundance: Rethinking How We Pay for Health CareEvaluare: 3.5 din 5 stele3.5/5 (2)
- Health Insurance Sector in India: A Study: Haldia Institute of Management, Haldia, West Bengal, IndiaDocument11 paginiHealth Insurance Sector in India: A Study: Haldia Institute of Management, Haldia, West Bengal, IndiaPanimalar Engineering College MBAÎncă nu există evaluări
- ChisDocument34 paginiChisAnagha MaryÎncă nu există evaluări
- The American Healthcare SystemDocument5 paginiThe American Healthcare SystemRajendra NurukurthiÎncă nu există evaluări
- HLTH 101Document7 paginiHLTH 101Yailine DlcÎncă nu există evaluări
- The Principle of Ethical JusticeDocument4 paginiThe Principle of Ethical JusticeJACKSON MULINGEÎncă nu există evaluări
- Finkelstein Etal Oregon 2012 PDFDocument50 paginiFinkelstein Etal Oregon 2012 PDFSamuel XiaoÎncă nu există evaluări
- Healthcare System of The United StatesDocument5 paginiHealthcare System of The United StatesjaredÎncă nu există evaluări
- It’s All About Money and Politics: Winning the Healthcare War: Your Guide to Healthcare ReformDe la EverandIt’s All About Money and Politics: Winning the Healthcare War: Your Guide to Healthcare ReformÎncă nu există evaluări
- Curing Australia's Health Care System: Reform by Joshua Gans and Stephen KingDocument27 paginiCuring Australia's Health Care System: Reform by Joshua Gans and Stephen KingCore ResearchÎncă nu există evaluări
- Argue EssayDocument3 paginiArgue Essayapi-740539255Încă nu există evaluări
- HLTH 101 Research PaperDocument9 paginiHLTH 101 Research Paperapi-566289467Încă nu există evaluări
- Finalengcomppaper AndrewsDocument13 paginiFinalengcomppaper Andrewsapi-583764833Încă nu există evaluări
- Living in the Shadow of Blackness as a Black Physician and Healthcare Disparity in the United States of AmericaDe la EverandLiving in the Shadow of Blackness as a Black Physician and Healthcare Disparity in the United States of AmericaÎncă nu există evaluări
- Health Insurance And Health Savings Account Made EasyDe la EverandHealth Insurance And Health Savings Account Made EasyÎncă nu există evaluări
- American Healthcare SystemDocument2 paginiAmerican Healthcare SystemFlorencia RodriguezÎncă nu există evaluări
- Health InsuranceDocument2 paginiHealth Insurancewilliam sunÎncă nu există evaluări
- DraftDocument4 paginiDraftapi-740539255Încă nu există evaluări
- Presentation On Health Care System ModelsDocument37 paginiPresentation On Health Care System ModelsTashi Makpen100% (1)
- Health Systems 2009 20aug ADocument74 paginiHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)Încă nu există evaluări
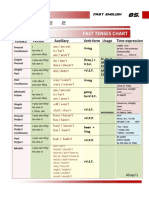
- Table 2: Fast Tenses ChartDocument5 paginiTable 2: Fast Tenses ChartAngel Julian HernandezÎncă nu există evaluări
- ICargo Mobility QantasDocument4 paginiICargo Mobility QantasViswateja KrottapalliÎncă nu există evaluări
- Mun Experience ProposalDocument2 paginiMun Experience Proposalapi-296978053Încă nu există evaluări
- SEBI Management Summary SheetsDocument398 paginiSEBI Management Summary SheetsPriyanka ChandakÎncă nu există evaluări
- DIS Investment ReportDocument1 paginăDIS Investment ReportHyperÎncă nu există evaluări
- Entrepreneurship: The Entrepreneur, The Individual That SteersDocument11 paginiEntrepreneurship: The Entrepreneur, The Individual That SteersJohn Paulo Sayo0% (1)
- 00 NamesDocument107 pagini00 Names朱奥晗Încă nu există evaluări
- Travel Services AgreementDocument36 paginiTravel Services AgreementEllijala VarunÎncă nu există evaluări
- Mormond History StudyDocument16 paginiMormond History StudyAndy SturdyÎncă nu există evaluări
- Impacts of Cultural Differences On Project SuccessDocument10 paginiImpacts of Cultural Differences On Project SuccessMichael OlaleyeÎncă nu există evaluări
- Specific Relief Act, 1963Document23 paginiSpecific Relief Act, 1963Saahiel Sharrma0% (1)
- CV2022095403 5222023 Minute EntryDocument6 paginiCV2022095403 5222023 Minute EntryJordan Conradson100% (2)
- Joseph Minh Van Phase in Teaching Plan Spring 2021Document3 paginiJoseph Minh Van Phase in Teaching Plan Spring 2021api-540705173Încă nu există evaluări
- 504 Loan Refinancing ProgramDocument5 pagini504 Loan Refinancing ProgramPropertywizzÎncă nu există evaluări
- Councils of Catholic ChurchDocument210 paginiCouncils of Catholic ChurchJoao Marcos Viana CostaÎncă nu există evaluări
- Chapter 6 Study GuideDocument3 paginiChapter 6 Study GuidejoeÎncă nu există evaluări
- Questionnaire of Personal and Organizational Values Congruence For Employee (Q-POVC-115)Document6 paginiQuestionnaire of Personal and Organizational Values Congruence For Employee (Q-POVC-115)Kowshik SÎncă nu există evaluări
- Satisfaction On Localized Services: A Basis of The Citizen-Driven Priority Action PlanDocument9 paginiSatisfaction On Localized Services: A Basis of The Citizen-Driven Priority Action PlanMary Rose Bragais OgayonÎncă nu există evaluări
- Principle Mining Economics01Document56 paginiPrinciple Mining Economics01Teddy Dkk100% (3)
- 1 s2.0 S0141391023000721 MainDocument28 pagini1 s2.0 S0141391023000721 MainYemey Quispe ParedesÎncă nu există evaluări
- La Bugal BLaan Tribal Association Inc. vs. RamosDocument62 paginiLa Bugal BLaan Tribal Association Inc. vs. RamosAKnownKneeMouseeÎncă nu există evaluări
- NEERJA 7th April 2016 Pre Shoot Draft PDFDocument120 paginiNEERJA 7th April 2016 Pre Shoot Draft PDFMuhammad Amir ShafiqÎncă nu există evaluări
- Yahoo Tabs AbbDocument85 paginiYahoo Tabs AbbKelli R. GrantÎncă nu există evaluări
- HRM in NestleDocument21 paginiHRM in NestleKrishna Jakhetiya100% (1)
- Relativity of ContractsDocument7 paginiRelativity of ContractsCristy C. Bangayan100% (1)
- ReadmeDocument2 paginiReadmeParthipan JayaramÎncă nu există evaluări
- 1 Summative Test in Empowerment Technology Name: - Date: - Year & Section: - ScoreDocument2 pagini1 Summative Test in Empowerment Technology Name: - Date: - Year & Section: - ScoreShelene CathlynÎncă nu există evaluări
- SIP REPORT Bindu PDFDocument61 paginiSIP REPORT Bindu PDFRahul HissariaÎncă nu există evaluări
- Flipkart Labels 23 Apr 2024 10 18Document4 paginiFlipkart Labels 23 Apr 2024 10 18Giri KanyakumariÎncă nu există evaluări
- CV - Parisi - UChileDocument5 paginiCV - Parisi - UChileFen_udechileÎncă nu există evaluări