S-ar putea să vă placă și
- Autonomous Robot-Aided Optical Manipulation for Biological CellsDe la EverandAutonomous Robot-Aided Optical Manipulation for Biological CellsÎncă nu există evaluări
- Pterygium: Surgical Techniques and ChoicesDocument2 paginiPterygium: Surgical Techniques and Choicespqwoeifjpakou134Încă nu există evaluări
- Fluorescence Microscopy: Super-Resolution and other Novel TechniquesDe la EverandFluorescence Microscopy: Super-Resolution and other Novel TechniquesAnda CorneaÎncă nu există evaluări
- Pterygium: Surgical Techniques and ChoicesDocument2 paginiPterygium: Surgical Techniques and ChoicesJohny Marquez TrochezÎncă nu există evaluări
- Electrosurgery in The Gastrointestinal Suite .4Document10 paginiElectrosurgery in The Gastrointestinal Suite .4Jesús MaríñezÎncă nu există evaluări
- Membranes: Past, Present and Future of Surgical Meshes: A ReviewDocument23 paginiMembranes: Past, Present and Future of Surgical Meshes: A Reviewdanis rafandra alkhalifiÎncă nu există evaluări
- Septal Extension Graft VS Collumellar StrutDocument8 paginiSeptal Extension Graft VS Collumellar Strutretribution499Încă nu există evaluări
- Biodegradable and Titanium Fixation Systems in Oral and Maxillofacial Surgery: A Randomized Controlled TrialDocument7 paginiBiodegradable and Titanium Fixation Systems in Oral and Maxillofacial Surgery: A Randomized Controlled TrialIene Dhiitta PramudÎncă nu există evaluări
- Does Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDocument6 paginiDoes Femoral Notching During Total Knee Arthroplasty Influence Periprosthetic Fracture. A Prospective StudyDavidBeatonComuladaÎncă nu există evaluări
- Application of Elastomeric Chains in OrtDocument5 paginiApplication of Elastomeric Chains in OrtEva ApriyaniÎncă nu există evaluări
- Lit Review Matrix For PocbpalDocument5 paginiLit Review Matrix For Pocbpalapi-403963757Încă nu există evaluări
- Nonlinear Elastic and Viscoelastic Deformation of The Human Red Blood Cell With Optical TweezersDocument12 paginiNonlinear Elastic and Viscoelastic Deformation of The Human Red Blood Cell With Optical TweezersDamoon5Încă nu există evaluări
- Comparison of Long-Term Surgical Outcomes of Two-Muscle Surgery in Basic-Type Intermittent Exotropia: Bilateral Versus UnilateralDocument9 paginiComparison of Long-Term Surgical Outcomes of Two-Muscle Surgery in Basic-Type Intermittent Exotropia: Bilateral Versus UnilateralerwinÎncă nu există evaluări
- 1 s2.0 S1877056812002769 MainDocument8 pagini1 s2.0 S1877056812002769 Mainmegawati vika pÎncă nu există evaluări
- Comparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessDocument6 paginiComparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessS3V4_9154Încă nu există evaluări
- International Journal of SurgeryDocument7 paginiInternational Journal of SurgeryJose Manuel Luna VazquezÎncă nu există evaluări
- Theoharidou A Et Al. 2008 (JOMI) PDFDocument10 paginiTheoharidou A Et Al. 2008 (JOMI) PDFAlla MushkeyÎncă nu există evaluări
- Europace 2009 Scott 1501 4Document4 paginiEuropace 2009 Scott 1501 4Matteo FranceschiniÎncă nu există evaluări
- Comparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsDocument7 paginiComparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsdianisaindiraÎncă nu există evaluări
- Systematic Review of Lesser Tuberosity Osteotomy Techniques Outcomes and Biomechanical Testing Parameters A Critical AppraisalDocument10 paginiSystematic Review of Lesser Tuberosity Osteotomy Techniques Outcomes and Biomechanical Testing Parameters A Critical AppraisalAthenaeum Scientific PublishersÎncă nu există evaluări
- Bloomberg 1989 (Advantages of Paramedian Approach)Document5 paginiBloomberg 1989 (Advantages of Paramedian Approach)Olivia LimÎncă nu există evaluări
- 223654-Article Text-546414-1-10-20220403Document6 pagini223654-Article Text-546414-1-10-20220403Christopher Freddy Bermeo RiveraÎncă nu există evaluări
- Annals of SurgeryDocument12 paginiAnnals of SurgeryNada GhammemÎncă nu există evaluări
- (2009 Kotsovilis) A Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental ImplantsDocument20 pagini(2009 Kotsovilis) A Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental Implantsyena1010Încă nu există evaluări
- Ceramic On Poly ImplantDocument8 paginiCeramic On Poly ImplantnithinvenkatÎncă nu există evaluări
- Management of Acquired Atresia of The External AudDocument5 paginiManagement of Acquired Atresia of The External AudgheaastridgayatriÎncă nu există evaluări
- 2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsDocument7 pagini2016 - Hand Transplantation Versus Hand Prosthetics - Pros and ConsMikiÎncă nu există evaluări
- Comparison of Polyetheretherketone Cables and Stainless Steel Wires For Sternal Fixation After Median SternotomyDocument8 paginiComparison of Polyetheretherketone Cables and Stainless Steel Wires For Sternal Fixation After Median SternotomyRafailiaÎncă nu există evaluări
- Comparative Evaluation of Healing After Gingivectomy With Electrocautery and LaserDocument7 paginiComparative Evaluation of Healing After Gingivectomy With Electrocautery and LaserWidy Seto UtomoÎncă nu există evaluări
- Tzimas Et Al 2022 Comparative Study of Surgical Wound Closure With Nylon Interrupted Sutures and Running SubcuticularDocument6 paginiTzimas Et Al 2022 Comparative Study of Surgical Wound Closure With Nylon Interrupted Sutures and Running SubcuticularVictor RomanÎncă nu există evaluări
- Applications of Digital Image Correlation To Biological TissuesDocument9 paginiApplications of Digital Image Correlation To Biological TissuesValeria NaranjoÎncă nu există evaluări
- Lateral Supraorbital Approach Vs Pterional Approach: An Anatomic Qualitative and Quantitative EvaluationDocument9 paginiLateral Supraorbital Approach Vs Pterional Approach: An Anatomic Qualitative and Quantitative EvaluationMartina javiera Alarcon AcevedoÎncă nu există evaluări
- Misra 2010Document9 paginiMisra 2010Fernando AraujoÎncă nu există evaluări
- Wide Diameter Implants-Degidi Piattelli LezziDocument7 paginiWide Diameter Implants-Degidi Piattelli LezziJing XueÎncă nu există evaluări
- Management of High-Energy Tibial Shaft Fractures Using The Hexapod Circular External FixatorDocument9 paginiManagement of High-Energy Tibial Shaft Fractures Using The Hexapod Circular External FixatorAlejandro OrduzÎncă nu există evaluări
- Surgical Therapy of Peri-ImplantitisDocument17 paginiSurgical Therapy of Peri-Implantitiskaue francoÎncă nu există evaluări
- THA Polyethylene SurvivalDocument5 paginiTHA Polyethylene SurvivalCleff FlowersÎncă nu există evaluări
- The Influence of Interimplant Distance and Attachment Type On The Retention Characteristics of MandiDocument7 paginiThe Influence of Interimplant Distance and Attachment Type On The Retention Characteristics of MandiNicco MarantsonÎncă nu există evaluări
- Journal Homepage: - : IntroductionDocument7 paginiJournal Homepage: - : IntroductionIJAR JOURNALÎncă nu există evaluări
- Surgical Treatment of Anterior Urethral Stricture DiseasesDocument9 paginiSurgical Treatment of Anterior Urethral Stricture DiseasesOmomomo781Încă nu există evaluări
- Dielectric Properties of Breast Carcinoma and The Surrounding TissuesDocument7 paginiDielectric Properties of Breast Carcinoma and The Surrounding TissuesPriya HankareÎncă nu există evaluări
- Poster 65: Exsanguinating Hemorrhage Following Third Molar ExtractionDocument2 paginiPoster 65: Exsanguinating Hemorrhage Following Third Molar ExtractionBhanu SatyanarayanaÎncă nu există evaluări
- Prosthetic Repair of Acutely Incarcerated Groin Hernias: A Prospective Clinical Observational Cohort StudyDocument6 paginiProsthetic Repair of Acutely Incarcerated Groin Hernias: A Prospective Clinical Observational Cohort Studynh2411Încă nu există evaluări
- Zygomatic ImplantDocument18 paginiZygomatic ImplantsmritinarayanÎncă nu există evaluări
- Image Guided Retrieval of Foreign Body As A Bail Out ProcedureDocument7 paginiImage Guided Retrieval of Foreign Body As A Bail Out ProcedureBIOMEDSCIDIRECT PUBLICATIONSÎncă nu există evaluări
- Coronectomy 2Document14 paginiCoronectomy 2Rovian RosaliaÎncă nu există evaluări
- Survey On Retention Protocols Among Turkish Orthodontists: Original ArticleDocument8 paginiSurvey On Retention Protocols Among Turkish Orthodontists: Original ArticleRebin AliÎncă nu există evaluări
- Zygomatic Implants PDFDocument18 paginiZygomatic Implants PDFgirl33Încă nu există evaluări
- (18915469 - Journal of Electrical Bioimpedance) Applications of Bioimpedance Measurement Techniques in Tissue EngineeringDocument17 pagini(18915469 - Journal of Electrical Bioimpedance) Applications of Bioimpedance Measurement Techniques in Tissue EngineeringgpaivÎncă nu există evaluări
- Protesis 15Document9 paginiProtesis 15ana márquezÎncă nu există evaluări
- Attachment Systems For Implant Retained Overdentures: A Literature ReviewDocument11 paginiAttachment Systems For Implant Retained Overdentures: A Literature ReviewpalliÎncă nu există evaluări
- Impedance Spectroscopy As A Tool For Monitoring Performance in 3D Models of Epithelial TissuesDocument16 paginiImpedance Spectroscopy As A Tool For Monitoring Performance in 3D Models of Epithelial TissuesgpaivÎncă nu există evaluări
- 1 s2.0 S2049080118300967 MainDocument4 pagini1 s2.0 S2049080118300967 MainNikhilesh GowdaÎncă nu există evaluări
- Platelet-Rich Fibrin Enhances Wound Epithelialization in The Skin Graft Donor SiteDocument9 paginiPlatelet-Rich Fibrin Enhances Wound Epithelialization in The Skin Graft Donor Siteyanuararipratama89Încă nu există evaluări
- Engineering A Highly Elastic Human Protien Based Sealant For Surgical ApplicationsDocument15 paginiEngineering A Highly Elastic Human Protien Based Sealant For Surgical ApplicationsKamonashis HalderÎncă nu există evaluări
- Root Cementum Part 11Document8 paginiRoot Cementum Part 11Sumedha MalshetwarÎncă nu există evaluări
- Mozzati 2013Document9 paginiMozzati 2013Larissa RodovalhoÎncă nu există evaluări
- Implantes en InmunosuprimidosDocument8 paginiImplantes en InmunosuprimidosLeandro PeraltaÎncă nu există evaluări
- Comparison Among Perfect-C®, Zero-P®, and Plates With A Cage in Single-Level Cervical Degenerative Disc DiseaseDocument10 paginiComparison Among Perfect-C®, Zero-P®, and Plates With A Cage in Single-Level Cervical Degenerative Disc DiseaseAleksandar DimovskiÎncă nu există evaluări
- Two Years Outcome of Cemented Austin Moore HemiartDocument7 paginiTwo Years Outcome of Cemented Austin Moore HemiartIkram HussainÎncă nu există evaluări
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 paginiDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanÎncă nu există evaluări
- Different Types of Tooth PreparationDocument56 paginiDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Support in Complete DentureDocument30 paginiSupport in Complete DentureSahana Rangarajan100% (2)
- Mandibular MovementDocument56 paginiMandibular MovementSahana RangarajanÎncă nu există evaluări
- Support in Complete DentureDocument16 paginiSupport in Complete DentureSahana RangarajanÎncă nu există evaluări
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 paginiFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanÎncă nu există evaluări
- Fulltext - Jda v5 Id1107Document3 paginiFulltext - Jda v5 Id1107Sahana RangarajanÎncă nu există evaluări
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pagini3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanÎncă nu există evaluări
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 paginiFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanÎncă nu există evaluări
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 paginiClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanÎncă nu există evaluări
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pagini6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanÎncă nu există evaluări
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 paginiA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanÎncă nu există evaluări
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pagini7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanÎncă nu există evaluări
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 paginiLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanÎncă nu există evaluări
- Mouth Guards in Dentistry-A Review: September 2018Document6 paginiMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanÎncă nu există evaluări
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 paginiReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanÎncă nu există evaluări
- 7 RetainerinorthodonticsDocument6 pagini7 RetainerinorthodonticsSahana RangarajanÎncă nu există evaluări
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 paginiElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanÎncă nu există evaluări
- Sauser 1957Document9 paginiSauser 1957Sahana RangarajanÎncă nu există evaluări
- Significance of Facebow For Dental RestorationsDocument5 paginiSignificance of Facebow For Dental RestorationsSahana RangarajanÎncă nu există evaluări
- Gothic Arch TrachingDocument7 paginiGothic Arch TrachingSahana RangarajanÎncă nu există evaluări
- Occlusion in Complete DentureDocument57 paginiOcclusion in Complete DentureSahana Rangarajan100% (1)
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 paginiProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanÎncă nu există evaluări
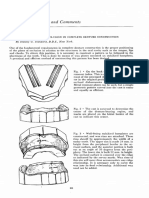
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 paginiCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanÎncă nu există evaluări
- The Anglo American Legal Concepts and Legal TerminologyDocument237 paginiThe Anglo American Legal Concepts and Legal TerminologyZviagin & CoÎncă nu există evaluări
- Mutilation AcquittalDocument2 paginiMutilation AcquittalKacel CastroÎncă nu există evaluări
- Every Step A Lotus Shoes For Bound Feet PDFDocument2 paginiEvery Step A Lotus Shoes For Bound Feet PDFKevinÎncă nu există evaluări
- Theories and Forms of Punishment 1Document48 paginiTheories and Forms of Punishment 1Jaspal KaurÎncă nu există evaluări
- Sterilization MutilationDocument21 paginiSterilization MutilationSheena De JesusÎncă nu există evaluări
- Mutilation JurisprudenceDocument2 paginiMutilation JurisprudenceMaria Cecilia MaquirangÎncă nu există evaluări
- Ateneo Central Criminal Law: Bar Operations 2020/21Document18 paginiAteneo Central Criminal Law: Bar Operations 2020/21Yec YecÎncă nu există evaluări
- History of Correction System 1 PDFDocument495 paginiHistory of Correction System 1 PDFArjhade SaritaÎncă nu există evaluări
- Simple Limb Prosthesis Process BookDocument39 paginiSimple Limb Prosthesis Process BookKyle McCormickÎncă nu există evaluări
- Module Crim Law IiDocument21 paginiModule Crim Law IiMaricar MendozaÎncă nu există evaluări
- Daftar Alat-Alat Skill Lab: No Nama Alat No - Katalog - Merk Gambar Total Harga (RP) Qty Harga Satuan (RP)Document4 paginiDaftar Alat-Alat Skill Lab: No Nama Alat No - Katalog - Merk Gambar Total Harga (RP) Qty Harga Satuan (RP)fk unramÎncă nu există evaluări
- Crime Elements Penalty Notes: Art. 262. Mutilation Intent Is To Specifically To CastrateDocument6 paginiCrime Elements Penalty Notes: Art. 262. Mutilation Intent Is To Specifically To CastrateZan BillonesÎncă nu există evaluări
- Physical InjuriesDocument5 paginiPhysical InjuriesEmrico CabahugÎncă nu există evaluări
- Female Genital MutilationDocument9 paginiFemale Genital Mutilationsh1508Încă nu există evaluări
- Crim 2Document18 paginiCrim 2paoloÎncă nu există evaluări
- Aguirre V Secretary of JusticeDocument2 paginiAguirre V Secretary of JusticeKacel Castro100% (1)
- Criminal Law 2Document79 paginiCriminal Law 2aris apridÎncă nu există evaluări
- Institutional Correction Review NoteDocument14 paginiInstitutional Correction Review NotePrincess Lee Guiali100% (1)
- Resumo Banestorm - An Abbreviated History of YrthDocument10 paginiResumo Banestorm - An Abbreviated History of YrthPortugalbino LopesÎncă nu există evaluări
- Ca1 HandoutsDocument4 paginiCa1 HandoutsJolliveen I. TacogdoyÎncă nu există evaluări
- Art 262 - 266Document21 paginiArt 262 - 266Dane Pauline AdoraÎncă nu există evaluări
- Module 10 Physical InjuriesDocument3 paginiModule 10 Physical InjuriesAngela ConejeroÎncă nu există evaluări
- MRRS Protocol and GCRVsDocument47 paginiMRRS Protocol and GCRVsRoh MihÎncă nu există evaluări
- Module Number 1: Crimes Against Persons Are Classified Into Three General CategoriesDocument21 paginiModule Number 1: Crimes Against Persons Are Classified Into Three General CategoriesMaricar MendozaÎncă nu există evaluări
- Decaptação e Esquartejamento de Um Corpo - Caso MatricidaDocument4 paginiDecaptação e Esquartejamento de Um Corpo - Caso MatricidaGabriel GabrielÎncă nu există evaluări
- Return Invoice 231.8.2023Document2 paginiReturn Invoice 231.8.2023ahmed.zulkhaireÎncă nu există evaluări
- PEQDocument39 paginiPEQdwi setyawanÎncă nu există evaluări
- Notes in Criminal Law II - Title 8Document13 paginiNotes in Criminal Law II - Title 8Jose Dula IIÎncă nu există evaluări
- Genocide of Women in HinduismDocument75 paginiGenocide of Women in Hinduismhan_chinese100% (1)
- Preliminary Ca 101Document9 paginiPreliminary Ca 101ShyyÎncă nu există evaluări
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 4.5 din 5 stele4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDe la EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesEvaluare: 4.5 din 5 stele4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 4 din 5 stele4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4.5 din 5 stele4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDe la EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsEvaluare: 4.5 din 5 stele4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDe la EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingEvaluare: 4 din 5 stele4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)