S-ar putea să vă placă și
- IBS ResearchDocument5 paginiIBS ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- An Open-Label Prospective Clinical Study To EvaluaDocument5 paginiAn Open-Label Prospective Clinical Study To Evaluamassleader251Încă nu există evaluări
- Park 2005Document9 paginiPark 2005Rina HerowatiÎncă nu există evaluări
- SR221214143625Document5 paginiSR221214143625Archana BiddikalÎncă nu există evaluări
- Clinical Evaluation of Purified Shilajit On TestosteroneDocument6 paginiClinical Evaluation of Purified Shilajit On TestosteroneAlejandro MüllerÎncă nu există evaluări
- Journalof Natural RemediesDocument10 paginiJournalof Natural RemediesAndreia TorresÎncă nu există evaluări
- Bhui Amla PPR PDFDocument2 paginiBhui Amla PPR PDFShazia FarooquiÎncă nu există evaluări
- Effects of Pushpadhanwa Rasa On Psychological Imbalances in Polycystic Ovarian Disease Patients and Its ManagementDocument8 paginiEffects of Pushpadhanwa Rasa On Psychological Imbalances in Polycystic Ovarian Disease Patients and Its ManagementabhishekÎncă nu există evaluări
- Standardization of Asanabilvadi Taila and BilvadilehaDocument78 paginiStandardization of Asanabilvadi Taila and BilvadilehaOctavian PlayzÎncă nu există evaluări
- A Review On Analytical Studies and Pharmacological Evaluation of Polyherbal FormulationsDocument13 paginiA Review On Analytical Studies and Pharmacological Evaluation of Polyherbal FormulationsIJAR JOURNALÎncă nu există evaluări
- Research Article: Management of Amavata (Rheumatoid Arthritis) by Application of Ayurvedic PrincipleDocument6 paginiResearch Article: Management of Amavata (Rheumatoid Arthritis) by Application of Ayurvedic PrinciplerajrajÎncă nu există evaluări
- 1334 PDFDocument3 pagini1334 PDFडा. सत्यदेव त्यागी आर्यÎncă nu există evaluări
- PCOS AyurvedaDocument9 paginiPCOS Ayurvedanaga chaitanyaÎncă nu există evaluări
- Book - Classical Ayurvedic Prescriptions For Common DiseasesDocument167 paginiBook - Classical Ayurvedic Prescriptions For Common DiseasesJhon Jairo Mosquera Rodas100% (3)
- 472-Article Text-1092-1-10-20200520Document4 pagini472-Article Text-1092-1-10-20200520asmita sainiÎncă nu există evaluări
- Cellular and Molecular Mechanisms of Curcumin in Prevention and Treatment of DiseaseDocument55 paginiCellular and Molecular Mechanisms of Curcumin in Prevention and Treatment of DiseaseJorge Luis Plasencia CubaÎncă nu există evaluări
- Jahm 201951 03Document3 paginiJahm 201951 03Vilas BhuwadÎncă nu există evaluări
- Exploratory Study To Evaluate Tolerability SafetyDocument4 paginiExploratory Study To Evaluate Tolerability Safetycini jerÎncă nu există evaluări
- Jie 4 118Document7 paginiJie 4 118200742 Elya AmaliaÎncă nu există evaluări
- Guidelines and Screening Methods of PharmacologyDe la EverandGuidelines and Screening Methods of PharmacologyÎncă nu există evaluări
- Ayurvedic Intervention For Hepatobiliary Disorders Current Scenario Andfuture Prospect2Document6 paginiAyurvedic Intervention For Hepatobiliary Disorders Current Scenario Andfuture Prospect2Ramachandran RadhakrishnanÎncă nu există evaluări
- Koolwal Et Al 2019 L Arginine and Erectile DysfunctionDocument7 paginiKoolwal Et Al 2019 L Arginine and Erectile Dysfunctioncloude21Încă nu există evaluări
- Thyagarajan2002 - Medicinas Herbales para Enfermedades Del Higado en India PDFDocument7 paginiThyagarajan2002 - Medicinas Herbales para Enfermedades Del Higado en India PDFEmmanuel GarcíaÎncă nu există evaluări
- Use of Probiotics For Management of Acute.30Document9 paginiUse of Probiotics For Management of Acute.30veren00Încă nu există evaluări
- Assessment of The Efficacy of Surya Namaskar in Management of SthaulyaDocument10 paginiAssessment of The Efficacy of Surya Namaskar in Management of Sthaulyans.saiprashanthÎncă nu există evaluări
- Evidence-Based Practice in Complementary and Alternative Medicine: Perspectives, Protocols, Problems and Potential in AyurvedaDe la EverandEvidence-Based Practice in Complementary and Alternative Medicine: Perspectives, Protocols, Problems and Potential in AyurvedaSanjeev RastogiÎncă nu există evaluări
- Arunkumar B. Biradar IJAMY-Volume 7 Number 3 Jul-Sep 2014 - 1589Document9 paginiArunkumar B. Biradar IJAMY-Volume 7 Number 3 Jul-Sep 2014 - 1589naga chaitanyaÎncă nu există evaluări
- Hypno 7Document11 paginiHypno 7Eka AfriliaÎncă nu există evaluări
- 972 ArticleText 4427 1 10 20220513Document8 pagini972 ArticleText 4427 1 10 20220513Andreia TorresÎncă nu există evaluări
- Art. 4 - 921Document6 paginiArt. 4 - 921aviralÎncă nu există evaluări
- Role of Picchavasthi in The Management of Grahani W.S.R Irritable Bowel SyndromeDocument4 paginiRole of Picchavasthi in The Management of Grahani W.S.R Irritable Bowel SyndromeDrHassan Ahmed ShaikhÎncă nu există evaluări
- Lobsang PDFDocument6 paginiLobsang PDFRohitÎncă nu există evaluări
- The Quest For Evidence Based AyurvedaDocument12 paginiThe Quest For Evidence Based Ayurvedaayurveda2011Încă nu există evaluări
- The Quest For Evidence-Based Ayurveda: Lessons Learned: Bhushan PatwardhanDocument13 paginiThe Quest For Evidence-Based Ayurveda: Lessons Learned: Bhushan PatwardhanJase HarrisonÎncă nu există evaluări
- 1 s2.0 S0975947617301158 Main PDFDocument5 pagini1 s2.0 S0975947617301158 Main PDFdanda1008716Încă nu există evaluări
- AyurpharmDocument8 paginiAyurpharmpalak GandhiÎncă nu există evaluări
- Original Article Ayurvedic Preparation in The Treatment of Nutritional AnemiaDocument8 paginiOriginal Article Ayurvedic Preparation in The Treatment of Nutritional AnemiaSundara VeerrajuÎncă nu există evaluări
- Efficacy and Tolerability of An Herbal Formulation For Weight ManagementDocument9 paginiEfficacy and Tolerability of An Herbal Formulation For Weight ManagementFaradina Zulaili Ifa EvendyÎncă nu există evaluări
- Bhattacharyya Et Al. 2008 - Etude Clinique Tulsi StressDocument5 paginiBhattacharyya Et Al. 2008 - Etude Clinique Tulsi StressSébastien Le QuéréÎncă nu există evaluări
- A Review of Research Papers On Nasya Karma in Cervical Spondylosis Published During 2010-2020Document11 paginiA Review of Research Papers On Nasya Karma in Cervical Spondylosis Published During 2010-2020HARIKRISHNAN RÎncă nu există evaluări
- File 131Document8 paginiFile 131ysvbjiÎncă nu există evaluări
- A Placebo-Controlled Pilot Study of Adjunctive OlanzapineDocument6 paginiA Placebo-Controlled Pilot Study of Adjunctive OlanzapineloloasbÎncă nu există evaluări
- Moayyedi P The Effect of Fiber Supplementation On IrritableDocument8 paginiMoayyedi P The Effect of Fiber Supplementation On Irritableoliffasalma atthahirohÎncă nu există evaluări
- Jahm 201624 07 2Document7 paginiJahm 201624 07 2Ripunjoy GoswamiÎncă nu există evaluări
- An Ayurvedic Concept For PreventionDocument8 paginiAn Ayurvedic Concept For Preventionyadun mrÎncă nu există evaluări
- 2022 - Lingyu - Acupuncture For The Treatment of Diarrhea-Predominant - EcaDocument11 pagini2022 - Lingyu - Acupuncture For The Treatment of Diarrhea-Predominant - EcaesmargarÎncă nu există evaluări
- Article WJPR 1402746141Document12 paginiArticle WJPR 1402746141Sahil MehtaÎncă nu există evaluări
- Pharmacovigilance Study of Ayurvedic Medicine in Ayurvedic Teaching Hospital: A Prospective Survey StudyDocument8 paginiPharmacovigilance Study of Ayurvedic Medicine in Ayurvedic Teaching Hospital: A Prospective Survey Studyfarhan akhtarÎncă nu există evaluări
- Paper Prueba RasayamDocument6 paginiPaper Prueba RasayamCARLOS HUMBERTO OVIEDO SANABRIAÎncă nu există evaluări
- Junaid Plag CheckDocument49 paginiJunaid Plag Checkjunaid nawazÎncă nu există evaluări
- Anticonvulsant Potential of Commonly Practiced Formulations of Brahmi (Bacopa Monnieri Linn.) in Wistar RatsDocument5 paginiAnticonvulsant Potential of Commonly Practiced Formulations of Brahmi (Bacopa Monnieri Linn.) in Wistar RatsHildayatiÎncă nu există evaluări
- Review of Ayurvedic Treatment of Menoraghea PDFDocument4 paginiReview of Ayurvedic Treatment of Menoraghea PDFNDSÎncă nu există evaluări
- A Study On Effect of Nimba Taila in The ManagementDocument5 paginiA Study On Effect of Nimba Taila in The Managementjssamc prasootitantraÎncă nu există evaluări
- Boswellia SerrataDocument5 paginiBoswellia Serrataluis fazendaÎncă nu există evaluări
- Role of AnupanaDocument9 paginiRole of AnupanaBrad YantzerÎncă nu există evaluări
- Effect and Interactions of Pueraria-Rehmannia and Aerobic Exercise On MetabolicDocument9 paginiEffect and Interactions of Pueraria-Rehmannia and Aerobic Exercise On Metabolicyhenti widjayantiÎncă nu există evaluări
- Classical Ayurvedic Prescriptions For Common Diseases (For Registered Ayurvedic Practitioners)Document167 paginiClassical Ayurvedic Prescriptions For Common Diseases (For Registered Ayurvedic Practitioners)greencrystal8189% (9)
- Ayurnutrigenomics Ayurveda-Inspired Personalized MedicineDocument7 paginiAyurnutrigenomics Ayurveda-Inspired Personalized MedicineSreedhar TirunagariÎncă nu există evaluări
- Covid - 19 & AyurvedaDocument34 paginiCovid - 19 & AyurvedaRajeev B PillaiÎncă nu există evaluări
- Autonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaDe la EverandAutonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaÎncă nu există evaluări
- Research A Comparative Clinical Study On The Effect of Some Compound Ayurvedic Preparations in The Management of Arsha-Ayur ResearchDocument14 paginiResearch A Comparative Clinical Study On The Effect of Some Compound Ayurvedic Preparations in The Management of Arsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Clinical Study On The Role of Ksara Vasti and Triphala Guggulu in Raktarsha-Ayur ResearchDocument4 paginiResearch A Clinical Study On The Role of Ksara Vasti and Triphala Guggulu in Raktarsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Comprative Study of Ksharkarma and Cryo Surgery in The Managment of Arsha (Haemorrhoids) - Ayur ResearchDocument7 paginiResearch A Comprative Study of Ksharkarma and Cryo Surgery in The Managment of Arsha (Haemorrhoids) - Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Review On Bheshaja Chikitsa in Arsha-Ayur ResearchDocument6 paginiResearch A Review On Bheshaja Chikitsa in Arsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Method in The Preparation of Teekshana Kshara and It's Practice in Haemorrhoids-Ayur ResearchDocument4 paginiResearch A Method in The Preparation of Teekshana Kshara and It's Practice in Haemorrhoids-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Comparative Study of Ksharsutra Ligation and Electro-Thermal Cautery in The Management of Arsha W. S. R. To Sentinel Piles-Ayur ResearchDocument11 paginiResearch A Comparative Study of Ksharsutra Ligation and Electro-Thermal Cautery in The Management of Arsha W. S. R. To Sentinel Piles-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- International Ayurvedic Medical Journal: Pardeshi Neetu NarayanDocument5 paginiInternational Ayurvedic Medical Journal: Pardeshi Neetu NarayanDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Clinical Study On The Role of Indigenous Formulation On Arsha-Ayur ResearchDocument8 paginiResearch A Clinical Study On The Role of Indigenous Formulation On Arsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Clinical Study of Kankayan Vati in The Management of Arshas-Ayur ResearchDocument5 paginiResearch A Clinical Study of Kankayan Vati in The Management of Arshas-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Comparative Clinical Study On Lavanottamadi Choorna and Chirabilwadi Choorna With Takra in The Management of Raktarsha-Ayur ResearchDocument8 paginiResearch A Comparative Clinical Study On Lavanottamadi Choorna and Chirabilwadi Choorna With Takra in The Management of Raktarsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- App Purchased With Expiry Date and Time LeftDocument3 paginiApp Purchased With Expiry Date and Time LeftDrHassan Ahmed ShaikhÎncă nu există evaluări
- A Prospective Study On Parpati Kalpana W.S.R To Panchamrut ParpatiDocument11 paginiA Prospective Study On Parpati Kalpana W.S.R To Panchamrut ParpatiDrHassan Ahmed ShaikhÎncă nu există evaluări
- Samples Sent For Testing Total Negative Reports Total Number of AdmissionsDocument1 paginăSamples Sent For Testing Total Negative Reports Total Number of AdmissionsDrHassan Ahmed ShaikhÎncă nu există evaluări
- Ayurvedic Management of Ulcerative Colitis W.S.R To Grahni Dusti-A Case StudyDocument6 paginiAyurvedic Management of Ulcerative Colitis W.S.R To Grahni Dusti-A Case StudyDrHassan Ahmed ShaikhÎncă nu există evaluări
- International Ayurvedic Medical Journal: CharacterizedDocument4 paginiInternational Ayurvedic Medical Journal: CharacterizedDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Clinical Study of Kutaja (Holarrhena Antidysenterica Wall) On Shonitarsha-Ayur ResearchDocument4 paginiResearch A Clinical Study of Kutaja (Holarrhena Antidysenterica Wall) On Shonitarsha-Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Research A Clinical Evalution of Efficacy of Certain Ayurvedic Formulations in The Management of Arsha (Haemorrhoids) - Ayur ResearchDocument16 paginiResearch A Clinical Evalution of Efficacy of Certain Ayurvedic Formulations in The Management of Arsha (Haemorrhoids) - Ayur ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- IBS ResearchDocument5 paginiIBS ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- IBS ResearchDocument6 paginiIBS ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- International Ayurvedic Medical Journal: Review Article ISSN: 2320 5091 Impact Factor: 5.344Document5 paginiInternational Ayurvedic Medical Journal: Review Article ISSN: 2320 5091 Impact Factor: 5.344DrHassan Ahmed ShaikhÎncă nu există evaluări
- Ayurveda Management of Ulcerative Colitis With Picchabasti: A Case StudyDocument3 paginiAyurveda Management of Ulcerative Colitis With Picchabasti: A Case StudyDrHassan Ahmed ShaikhÎncă nu există evaluări
- Role of Picchavasthi in The Management of Grahani W.S.R Irritable Bowel SyndromeDocument4 paginiRole of Picchavasthi in The Management of Grahani W.S.R Irritable Bowel SyndromeDrHassan Ahmed ShaikhÎncă nu există evaluări
- IBS ResearchDocument2 paginiIBS ResearchDrHassan Ahmed ShaikhÎncă nu există evaluări
- Clinical Study of Himanshwadi Churna in The Management of Vataj Grahani W.R.T. Irritable Bowel SyndromeDocument7 paginiClinical Study of Himanshwadi Churna in The Management of Vataj Grahani W.R.T. Irritable Bowel SyndromeDrHassan Ahmed ShaikhÎncă nu există evaluări
- Maharashtra (PGA CET 2007)Document23 paginiMaharashtra (PGA CET 2007)DrHassan Ahmed ShaikhÎncă nu există evaluări
- Maharashtra (PGA CET 2006)Document24 paginiMaharashtra (PGA CET 2006)DrHassan Ahmed ShaikhÎncă nu există evaluări
- Maharashtra (PGA CET 2014)Document49 paginiMaharashtra (PGA CET 2014)DrHassan Ahmed ShaikhÎncă nu există evaluări
- Physiology Model Test Papers New Updated 2016Document28 paginiPhysiology Model Test Papers New Updated 2016DrHassan Ahmed ShaikhÎncă nu există evaluări
- Maharashtra (PGA CET 2010)Document21 paginiMaharashtra (PGA CET 2010)DrHassan Ahmed ShaikhÎncă nu există evaluări
- Introduction To Laboratory Tests Handout VersionDocument58 paginiIntroduction To Laboratory Tests Handout VersionFiorellaBeatrizÎncă nu există evaluări
- B.Sc. Nsg. CurriculumDocument206 paginiB.Sc. Nsg. CurriculumPitambar PoudelÎncă nu există evaluări
- CCHM 311 Week 1617 Liver FunctionDocument10 paginiCCHM 311 Week 1617 Liver FunctionMax RuideraÎncă nu există evaluări
- Hepatoprotective Activity of Elytraria Acaulis in CCL4Document14 paginiHepatoprotective Activity of Elytraria Acaulis in CCL4Sudheer JayaramÎncă nu există evaluări
- Pemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)Document51 paginiPemeriksaan Fungsi Hati .: Prof. Dr. Adi Koesoema Aman SPPK (KH)kiki rawitriÎncă nu există evaluări
- All BioDocument2 paginiAll BioKpop 4th Gen EnjoyerÎncă nu există evaluări
- 10 Golden Rules in MedicationDocument2 pagini10 Golden Rules in MedicationYha Nha RhuÎncă nu există evaluări
- Infectious Diseases of The Dog and Cat, 3rd Edition: CHAPTER 90 Hepatobiliary InfectionsDocument47 paginiInfectious Diseases of The Dog and Cat, 3rd Edition: CHAPTER 90 Hepatobiliary InfectionssoledadDC329Încă nu există evaluări
- VotrientDocument29 paginiVotrientgini erwantiÎncă nu există evaluări
- ABCC ComACC Core Competencies CurriculumDocument29 paginiABCC ComACC Core Competencies CurriculumABDULLAH ALTURAIFÎncă nu există evaluări
- Diabetic Retinopathy As A Risk Factor Associated With The Development of Hepatocellular Carcinoma in Nonalcoholic Fatty Liver DiseaseDocument8 paginiDiabetic Retinopathy As A Risk Factor Associated With The Development of Hepatocellular Carcinoma in Nonalcoholic Fatty Liver DiseaseameliaÎncă nu există evaluări
- SGPT (Serum Glutamic-Pyruvic Transaminase), ALT (Alanine Aminotransferase), InterpretationsDocument55 paginiSGPT (Serum Glutamic-Pyruvic Transaminase), ALT (Alanine Aminotransferase), InterpretationsReman A. AlingasaÎncă nu există evaluări
- Hepatic Disease in PregnancyDocument37 paginiHepatic Disease in PregnancyElisha Joshi100% (1)
- Liver Function Lecture NotesDocument9 paginiLiver Function Lecture NotesMarie Bernadette DigoÎncă nu există evaluări
- Course Task 2Document2 paginiCourse Task 2John Elton TangpuzÎncă nu există evaluări
- Professor Dr. Najat A. HasanDocument40 paginiProfessor Dr. Najat A. HasanPeter MungaiÎncă nu există evaluări
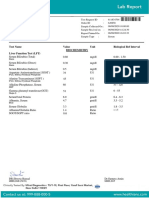
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Document7 paginiTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelÎncă nu există evaluări
- Medicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1Document120 paginiMedicine Alaa Notes (All Files Merged) - Best Pro Choice-.Pdf-1maimoona suleman100% (6)
- See Full Prescribing Information For Complete Boxed WarningDocument16 paginiSee Full Prescribing Information For Complete Boxed Warninggmsanto7Încă nu există evaluări
- Hepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Document10 paginiHepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Reddy LufyanÎncă nu există evaluări
- Chapter 6 PharmacologyDocument33 paginiChapter 6 Pharmacologym1k0eÎncă nu există evaluări
- Fibroza HepaticaDocument70 paginiFibroza HepaticairiscelÎncă nu există evaluări
- Chemistry - Cornell University College of Veterinary MedicineDocument2 paginiChemistry - Cornell University College of Veterinary MedicineMikaelle CastilhoÎncă nu există evaluări
- Normal Laboratory ValuesDocument4 paginiNormal Laboratory ValuesPaulene CartelÎncă nu există evaluări
- Acute Alcoholic HepatitisDocument18 paginiAcute Alcoholic HepatitisMariana NavarroÎncă nu există evaluări
- Enzymes Lacking Video 7Document16 paginiEnzymes Lacking Video 7Hanzel RebutaÎncă nu există evaluări
- Zainab Muhammad T.RDocument31 paginiZainab Muhammad T.RAdam AbubakarÎncă nu există evaluări
- Lab Value MnemonicsDocument10 paginiLab Value MnemonicsSophia CuertoÎncă nu există evaluări
- Newborn ProfileDocument92 paginiNewborn ProfilesarikaÎncă nu există evaluări
- CCII 8.0 - Clinical EnzymologyDocument2 paginiCCII 8.0 - Clinical EnzymologyWynlor AbarcaÎncă nu există evaluări