S-ar putea să vă placă și
- Anterior Cruciate Ligament-Injury & ManagementDocument101 paginiAnterior Cruciate Ligament-Injury & ManagementYusuf Brilliant100% (1)
- Trauma Musculoskeletal - Spine FKK UMJ1Document92 paginiTrauma Musculoskeletal - Spine FKK UMJ1Hendra Hash AwoÎncă nu există evaluări
- 04 Mediastinum, HeartDocument27 pagini04 Mediastinum, HeartShaira Aquino VerzosaÎncă nu există evaluări
- Biomechanics of The Anterior Cruciate LigamentDocument37 paginiBiomechanics of The Anterior Cruciate LigamentRoshynta Linggar Andatu100% (1)
- Concise Anatomy For Anaesthesia PDFDocument148 paginiConcise Anatomy For Anaesthesia PDFMa Lopez67% (3)
- Lower Limb FracturesDocument124 paginiLower Limb FracturesMaríaJosé Dip100% (3)
- Anterior Cruciate Ligament Tear DefinitionDocument8 paginiAnterior Cruciate Ligament Tear DefinitionEunice IquinaÎncă nu există evaluări
- SDSG Radiographic Measuremnt ManualDocument120 paginiSDSG Radiographic Measuremnt ManualYuliana Wiralestari100% (2)
- Rotator CuffDocument46 paginiRotator CuffLiza Perez- Pagatpatan100% (2)
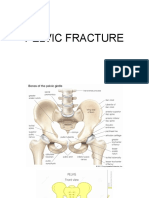
- Pelvic FractureDocument31 paginiPelvic Fracturepoe3Încă nu există evaluări
- Femoral Shaft FractureDocument44 paginiFemoral Shaft FracturePrabuddha ThihawaÎncă nu există evaluări
- OKU 5 Orthopaedic Knowledge Update SpineDocument45 paginiOKU 5 Orthopaedic Knowledge Update SpinePubMed77100% (1)
- Pelvi-Acetabular Fracture Treatment OverviewDocument136 paginiPelvi-Acetabular Fracture Treatment OverviewPicha PichiÎncă nu există evaluări
- Anatomy, Lecture 6, Pericardium and The Heart (Slides)Document22 paginiAnatomy, Lecture 6, Pericardium and The Heart (Slides)Ali Al-Qudsi100% (1)
- Type of IncisionsDocument5 paginiType of IncisionsChelzea ObarÎncă nu există evaluări
- Pelvic InjuriesDocument35 paginiPelvic InjuriesJavier Saad100% (1)
- Mechanism of Normal LabourDocument42 paginiMechanism of Normal Labourjayapreethiravi94% (18)
- Guidelines Made Simple 2017 HBPDocument28 paginiGuidelines Made Simple 2017 HBPThomas EipeÎncă nu există evaluări
- Pelvic Trauma: DR Indro Wibowo SejatiDocument42 paginiPelvic Trauma: DR Indro Wibowo SejatiIndro WibowoÎncă nu există evaluări
- Ortho Fraktur 1/3 Proximal Humerus DextraDocument57 paginiOrtho Fraktur 1/3 Proximal Humerus DextraFian ChristoÎncă nu există evaluări
- Musculoskeletal Disorders of Elbow, Wrist and HandsDocument59 paginiMusculoskeletal Disorders of Elbow, Wrist and Handssaroj yadavÎncă nu există evaluări
- PELVIC INJURY CAUSES, SIGNS AND TREATMENTDocument44 paginiPELVIC INJURY CAUSES, SIGNS AND TREATMENTabhishek chaudharyÎncă nu există evaluări
- Pelvic Fractures PksDocument48 paginiPelvic Fractures PksprinceveettoorÎncă nu există evaluări
- I. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Document42 paginiI. Dr. Yoyos - Unstable Pelvic Fracture Jam 14Rsud Malinau Ppk BludÎncă nu există evaluări
- Pelvic Fractures SubodhDocument131 paginiPelvic Fractures SubodhSubodh PathakÎncă nu există evaluări
- Pelvicinjuries 181026150723Document106 paginiPelvicinjuries 181026150723EntesipatyÎncă nu există evaluări
- Pelvic TraumaDocument20 paginiPelvic Traumachehak.kumar2000Încă nu există evaluări
- CR - RamirezDocument4 paginiCR - RamirezTommysÎncă nu există evaluări
- Life-Threatening Extremity and Pelvic InjuriesDocument41 paginiLife-Threatening Extremity and Pelvic Injuriesyuliaoksiyulanda ingeniopadangÎncă nu există evaluări
- Thoracolumbarfractures 150817055817 Lva1 App6891Document75 paginiThoracolumbarfractures 150817055817 Lva1 App6891Pap PipÎncă nu există evaluări
- Proximal Femur Fractures: Sulita Turaganiwai s130364Document26 paginiProximal Femur Fractures: Sulita Turaganiwai s130364Wālē NandÎncă nu există evaluări
- Adult FracturesDocument43 paginiAdult FracturesfujiÎncă nu există evaluări
- Case of Thoracic Outlet Syndrome - Cervical Rib: Presented and Discussed By: DR Praveen C.RDocument42 paginiCase of Thoracic Outlet Syndrome - Cervical Rib: Presented and Discussed By: DR Praveen C.RPraveen CrÎncă nu există evaluări
- Initial Management in Musculoskeletal Trauma: Yoyos D. IsmiartoDocument40 paginiInitial Management in Musculoskeletal Trauma: Yoyos D. IsmiartozaroziÎncă nu există evaluări
- Lower Extremity TraumaDocument72 paginiLower Extremity TraumaMariamÎncă nu există evaluări
- Pelvic Injury Dr. DarmajiDocument38 paginiPelvic Injury Dr. DarmajiAhmadNurwantoÎncă nu există evaluări
- LBM 4 - Signs, Classification, Diagnosis and Complications of Pelvic FracturesDocument6 paginiLBM 4 - Signs, Classification, Diagnosis and Complications of Pelvic FracturesindahsariÎncă nu există evaluări
- Dislocations (PDFDrive)Document111 paginiDislocations (PDFDrive)hemasary15Încă nu există evaluări
- Pelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaDocument46 paginiPelvic Trauma: Stud.: Andris Džeriņš, MF V 5.gr. Mentor: Dr. Med. Ruta JakušonokaRendy SusantoÎncă nu există evaluări
- Seminar on Managing Pelvic FracturesDocument89 paginiSeminar on Managing Pelvic FracturesAndreas RendraÎncă nu există evaluări
- Pelvic-Trauma - Traume PelvineDocument50 paginiPelvic-Trauma - Traume PelvineCristiana TanaseÎncă nu există evaluări
- Pelvic Fracture and Hip DislocationDocument62 paginiPelvic Fracture and Hip DislocationAbdulsalam DostÎncă nu există evaluări
- Shoulder and HumerusDocument75 paginiShoulder and HumerusIka HarikartiÎncă nu există evaluări
- Pelvis and HipDocument90 paginiPelvis and Hipalsead798Încă nu există evaluări
- Pelvictrauma 151103203943 Lva1 App6892Document40 paginiPelvictrauma 151103203943 Lva1 App6892Navin BalajiÎncă nu există evaluări
- Painful Shoulder Injury Case ReportDocument17 paginiPainful Shoulder Injury Case ReportinhaÎncă nu există evaluări
- Pelvic Fractures: Understanding High-EnergyDocument4 paginiPelvic Fractures: Understanding High-EnergyRiscky LauwÎncă nu există evaluări
- Spine and Spinal Cord Trauma GuideDocument29 paginiSpine and Spinal Cord Trauma Guideg3niu5Încă nu există evaluări
- CaseDocument31 paginiCaseNovitasariyantiÎncă nu există evaluări
- Acute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeDocument54 paginiAcute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeKiara GovenderÎncă nu există evaluări
- Pelvic Injruies 2Document57 paginiPelvic Injruies 2King salehÎncă nu există evaluări
- Anatomy, Radiographic Evaluation, and Classification of Pelvic Ring InjuriesDocument83 paginiAnatomy, Radiographic Evaluation, and Classification of Pelvic Ring InjuriesClever ImaniaÎncă nu există evaluări
- Closed Fracture of Left Femoral Neck: Case ReportDocument31 paginiClosed Fracture of Left Femoral Neck: Case Reporttari nurulÎncă nu există evaluări
- Pelvic Ring InjuriesDocument11 paginiPelvic Ring InjuriesTegar Jati KusumaÎncă nu există evaluări
- Pelvic Fractures - These Can Kill YouDocument20 paginiPelvic Fractures - These Can Kill YouSurgicalgownÎncă nu există evaluări
- Revascularization Treatment For The Individual With PADDocument28 paginiRevascularization Treatment For The Individual With PADAnonymous qSWfAzt59gÎncă nu există evaluări
- RTC Brachial Artery Injury and Upper Ext FasciotomyDocument47 paginiRTC Brachial Artery Injury and Upper Ext FasciotomyAndini RezkiÎncă nu există evaluări
- Hip Dislocation-Ortho Topic PresentationDocument44 paginiHip Dislocation-Ortho Topic PresentationRachata PiriyamanunÎncă nu există evaluări
- Trauma Pelvic With Rectum InjuriesDocument91 paginiTrauma Pelvic With Rectum InjuriesAditya Wirakarna100% (1)
- GUS CASE 5 - Fraktur PelvisDocument18 paginiGUS CASE 5 - Fraktur PelvisCassantha papjiÎncă nu există evaluări
- DD Case Report Elbow DislocationDocument33 paginiDD Case Report Elbow DislocationKurniawan Nur IhsanÎncă nu există evaluări
- Spinal Cord Injury: Andi IhwanDocument31 paginiSpinal Cord Injury: Andi IhwanAndi Muliana SultaniÎncă nu există evaluări
- Pelvic FractureDocument18 paginiPelvic FractureTantyaÎncă nu există evaluări
- Scapular Dyskinesis and SICK Scapula Syndrome in Patients With Chronic Type III Acromioclavicular DislocationDocument6 paginiScapular Dyskinesis and SICK Scapula Syndrome in Patients With Chronic Type III Acromioclavicular DislocationNico BrantesÎncă nu există evaluări
- Subaxial Cervical FX VIDocument40 paginiSubaxial Cervical FX VIvicky174Încă nu există evaluări
- Acetabular FractureDocument4 paginiAcetabular FractureHossein VakiliÎncă nu există evaluări
- Acute Surgical Topics: An Infographic GuideDe la EverandAcute Surgical Topics: An Infographic GuideÎncă nu există evaluări
- Willow 44Document19 paginiWillow 44jackie funtanillaÎncă nu există evaluări
- WillowDocument14 paginiWillowjackie funtanillaÎncă nu există evaluări
- Willow 33Document18 paginiWillow 33jackie funtanillaÎncă nu există evaluări
- Doc01 - Copy333Document11 paginiDoc01 - Copy333jackie funtanillaÎncă nu există evaluări
- Doc01 - Copy333Document12 paginiDoc01 - Copy333jackie funtanillaÎncă nu există evaluări
- WillowDocument14 paginiWillowjackie funtanillaÎncă nu există evaluări
- Doc01 - Copy333Document12 paginiDoc01 - Copy333jackie funtanillaÎncă nu există evaluări
- Doc01 - Copy22Document7 paginiDoc01 - Copy22jackie funtanillaÎncă nu există evaluări
- Initiation of Antihypertensive Therapy Based On.480Document2 paginiInitiation of Antihypertensive Therapy Based On.480jackie funtanillaÎncă nu există evaluări
- Preterm birth risks and preventionDocument4 paginiPreterm birth risks and preventionjackie funtanillaÎncă nu există evaluări
- Doc01 - Copy333Document10 paginiDoc01 - Copy333jackie funtanillaÎncă nu există evaluări
- Optimizing Hypertension PDFDocument1 paginăOptimizing Hypertension PDFjackie funtanillaÎncă nu există evaluări
- Clinical Practice Guidelines For The Management of HypertensionDocument13 paginiClinical Practice Guidelines For The Management of HypertensionDaniel Opazo DamianiÎncă nu există evaluări
- 01Document4 pagini01jackie funtanillaÎncă nu există evaluări
- Initiation of Antihypertensive Therapy Based On.480Document2 paginiInitiation of Antihypertensive Therapy Based On.480jackie funtanillaÎncă nu există evaluări
- 11CPG-Management of Sore ThroatDocument26 pagini11CPG-Management of Sore ThroatmakeitrealityÎncă nu există evaluări
- Initiation of Antihypertensive Therapy Based On.480Document2 paginiInitiation of Antihypertensive Therapy Based On.480jackie funtanillaÎncă nu există evaluări
- PSYCHIATRY 1.1 Signs Symptoms of Mental Illness PDFDocument3 paginiPSYCHIATRY 1.1 Signs Symptoms of Mental Illness PDFjackie funtanillaÎncă nu există evaluări
- 11CPG-Management of Sore ThroatDocument26 pagini11CPG-Management of Sore ThroatmakeitrealityÎncă nu există evaluări
- Philippine Society of Otolaryngology-Head and Neck Surgery, Inc.-Task Force On Clinical Practice GuideDocument16 paginiPhilippine Society of Otolaryngology-Head and Neck Surgery, Inc.-Task Force On Clinical Practice GuideAljon S. TemploÎncă nu există evaluări
- Laboratory ResultsDocument4 paginiLaboratory Resultsjackie funtanillaÎncă nu există evaluări
- Sodium and Potassium Intake in Overweight And.596Document2 paginiSodium and Potassium Intake in Overweight And.596jackie funtanillaÎncă nu există evaluări
- 11CPG-Management of Sore ThroatDocument26 pagini11CPG-Management of Sore ThroatmakeitrealityÎncă nu există evaluări
- Initiation of Antihypertensive Therapy Based On.480Document2 paginiInitiation of Antihypertensive Therapy Based On.480jackie funtanillaÎncă nu există evaluări
- Hypertensive Urgency PDFDocument48 paginiHypertensive Urgency PDFjackie funtanillaÎncă nu există evaluări
- Optimizing Hypertension Management in Renal.28Document1 paginăOptimizing Hypertension Management in Renal.28jackie funtanillaÎncă nu există evaluări
- Simplifying Lab Test InterpretationDocument36 paginiSimplifying Lab Test Interpretationjackie funtanillaÎncă nu există evaluări
- Medical Ethics - ConceptsDocument39 paginiMedical Ethics - Conceptsjackie funtanillaÎncă nu există evaluări
- Heartbeat Sequencing Colour by NumbersDocument5 paginiHeartbeat Sequencing Colour by NumbersKavs KitchensÎncă nu există evaluări
- Abdomen CAP Questions and AnswersDocument6 paginiAbdomen CAP Questions and AnswersRathnaÎncă nu există evaluări
- Diaphragm AnatomyDocument19 paginiDiaphragm AnatomyasujithdrÎncă nu există evaluări
- Pelvic Floor Rehab Relieves Chronic Coccyx PainDocument1 paginăPelvic Floor Rehab Relieves Chronic Coccyx PainVizaÎncă nu există evaluări
- Dr. Meidona - Development of Gastrointestinal System PDFDocument54 paginiDr. Meidona - Development of Gastrointestinal System PDFwkwkwkhhhhÎncă nu există evaluări
- Introduction Abdomen DR 130818235819 Phpapp02Document11 paginiIntroduction Abdomen DR 130818235819 Phpapp02Namrata GabaÎncă nu există evaluări
- Radioanatomi Jantung Kel 9bDocument42 paginiRadioanatomi Jantung Kel 9bMuhamad KeanuÎncă nu există evaluări
- Yusi - Anatomy of The Urinary Tract 2009 12-7Document129 paginiYusi - Anatomy of The Urinary Tract 2009 12-7abstabsÎncă nu există evaluări
- Functional Anatomy of the Core as a Flexible CylinderDocument6 paginiFunctional Anatomy of the Core as a Flexible Cylinderarold bodoÎncă nu există evaluări
- Hasil Anatomi AvesDocument7 paginiHasil Anatomi AvesFriska nur shintiaÎncă nu există evaluări
- Neutral vs Imprint: Why Neutral Is Best for PilatesDocument2 paginiNeutral vs Imprint: Why Neutral Is Best for PilatesDance For Fitness With PoojaÎncă nu există evaluări
- Tugas Koding: Merlindi HestiaraDocument9 paginiTugas Koding: Merlindi HestiaraShafiaÎncă nu există evaluări
- The Respiratory SystemDocument6 paginiThe Respiratory SystemIftikharÎncă nu există evaluări
- Осев скелетDocument38 paginiОсев скелетEmma DanovaÎncă nu există evaluări
- Allreports PDFDocument2 paginiAllreports PDFNeena SinghÎncă nu există evaluări
- Sonography ReportDocument1 paginăSonography ReportChirag solankiÎncă nu există evaluări
- Archiv Euromedica 06 2021 001 126 16 01 2022 13Document6 paginiArchiv Euromedica 06 2021 001 126 16 01 2022 13Georgiana BuneaÎncă nu există evaluări
- PM&R in Degenearative Joint DiseaseDocument66 paginiPM&R in Degenearative Joint DiseaseLorenz SmallÎncă nu există evaluări
- Anatomy TermsDocument1 paginăAnatomy TermsStephanie MolinaÎncă nu există evaluări
- Frog Digestive SystemDocument2 paginiFrog Digestive SystemNiezhel Anne JimenezÎncă nu există evaluări
- Coccyx PDFDocument5 paginiCoccyx PDFtechzonesÎncă nu există evaluări
- Sklera Sub IkterikDocument7 paginiSklera Sub IkterikFauziah_Hannum_SÎncă nu există evaluări
- Posterior Abdominal Wall AnatomyDocument41 paginiPosterior Abdominal Wall AnatomypashaÎncă nu există evaluări