S-ar putea să vă placă și
- Free Medical ECG Interpretation PresentationsDocument30 paginiFree Medical ECG Interpretation PresentationsRohini SelvarajahÎncă nu există evaluări
- Study of Pediatric Congenital Cardiac Malformations by EchocardiographyDocument23 paginiStudy of Pediatric Congenital Cardiac Malformations by EchocardiographyRana Abd AlmugeethÎncă nu există evaluări
- Cardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyDocument87 paginiCardiology/EKG Board Review: Michael J. Bradley D.O. DME/Program Director Family Medicine ResidencyummimalikihamidÎncă nu există evaluări
- Hepatic Vein FlowDocument14 paginiHepatic Vein FlowJORGEÎncă nu există evaluări
- Aortic Root & Ascending Aortic Aneurysm Surgery OptionsTITLEDocument82 paginiAortic Root & Ascending Aortic Aneurysm Surgery OptionsTITLEMustafa KamalÎncă nu există evaluări
- The Heart: A Dual Pump and Rhythmic MuscleDocument10 paginiThe Heart: A Dual Pump and Rhythmic Muscle22194Încă nu există evaluări
- ELECTROCARDIOGRAPHY IN ISCHEMIC HEART DISEASEDe la EverandELECTROCARDIOGRAPHY IN ISCHEMIC HEART DISEASEÎncă nu există evaluări
- BradyarrthmiaDocument73 paginiBradyarrthmiaKuba ArebaÎncă nu există evaluări
- ECG IMM 2020.docx.2Document25 paginiECG IMM 2020.docx.2Abdul QuyyumÎncă nu există evaluări
- Bundle Branch Block ECG ChangesDocument47 paginiBundle Branch Block ECG Changesdragon66Încă nu există evaluări
- Aortic ExamDocument3 paginiAortic ExamReda SoÎncă nu există evaluări
- Mitral Valve Prolapse, A Simple Guide to The Condition, Treatment And Related ConditionsDe la EverandMitral Valve Prolapse, A Simple Guide to The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- Care of The Patient With A Cardiac Mechanical DisorderDocument8 paginiCare of The Patient With A Cardiac Mechanical DisorderthubtendrolmaÎncă nu există evaluări
- Financial MarketsDocument323 paginiFinancial MarketsSetu Ahuja100% (2)
- ECG Learning ModulesDocument150 paginiECG Learning ModulesdodiÎncă nu există evaluări
- EKG Strips For Posttest Questions 14-20Document3 paginiEKG Strips For Posttest Questions 14-20Aņņå SëiŗÿúùÎncă nu există evaluări
- Advanced Knowledge Assessment in Adult Critical CareDocument570 paginiAdvanced Knowledge Assessment in Adult Critical CareMajor EmadÎncă nu există evaluări
- Atrial Septial DefectDocument22 paginiAtrial Septial DefectJulie MckinneyÎncă nu există evaluări
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookDe la EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookÎncă nu există evaluări
- 6 Strategies For Effective Financial Management Trends in K12 SchoolsDocument16 pagini6 Strategies For Effective Financial Management Trends in K12 SchoolsRainiel Victor M. CrisologoÎncă nu există evaluări
- Approach To Ventricular ArrhythmiasDocument18 paginiApproach To Ventricular ArrhythmiasDavid CruzÎncă nu există evaluări
- A Handbook of Aortoarteritis and Ruptured Sinus of ValsalvaDe la EverandA Handbook of Aortoarteritis and Ruptured Sinus of ValsalvaÎncă nu există evaluări
- Diseases of The AortaDocument48 paginiDiseases of The AortaYibeltal AssefaÎncă nu există evaluări
- Transcutaneous Pacing for BradyarrhythmiasDocument21 paginiTranscutaneous Pacing for Bradyarrhythmiasdragon66Încă nu există evaluări
- DirtyMobs' Ultimate Matchup GuideDocument5 paginiDirtyMobs' Ultimate Matchup GuideTempest JannaÎncă nu există evaluări
- Diastolic Dysfunction AssessmentDocument42 paginiDiastolic Dysfunction AssessmentMustajab MujtabaÎncă nu există evaluări
- AwsDocument8 paginiAwskiranÎncă nu există evaluări
- Left Ventricular Hypertrophy: Detection, Significance and TreatmentDocument27 paginiLeft Ventricular Hypertrophy: Detection, Significance and TreatmentKudor Szabadi ZoltánÎncă nu există evaluări
- ECG Flashcards: Atrial ArrhythmiasDocument27 paginiECG Flashcards: Atrial ArrhythmiasDima HabanjarÎncă nu există evaluări
- Adult Congenital Heart Disease Board ReviewDocument79 paginiAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnÎncă nu există evaluări
- Electrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument29 paginiElectrical Axis: Fast & Easy Ecgs - A Self-Paced Learning ProgramMihaela PrisacaruÎncă nu există evaluări
- Basics of Pacing CombinedDocument54 paginiBasics of Pacing CombinedMichael Susanto100% (1)
- The P WaveDocument13 paginiThe P Wave成失Încă nu există evaluări
- DR K Chan - Ecg For SVT Made EasyDocument66 paginiDR K Chan - Ecg For SVT Made Easyapi-346486620Încă nu există evaluări
- CARDIAC CYCLE New For StudentDocument54 paginiCARDIAC CYCLE New For StudentDavi DzikirianÎncă nu există evaluări
- Dysrhytmia NotesDocument11 paginiDysrhytmia NoteshannahhwolfÎncă nu există evaluări
- ECG Quiz Prep: Key Points for Interpreting RhythmsDocument7 paginiECG Quiz Prep: Key Points for Interpreting RhythmsAAÎncă nu există evaluări
- Pacing Week PresentationsDocument54 paginiPacing Week PresentationsjoejenningsÎncă nu există evaluări
- Prosth ValvesDocument74 paginiProsth ValvesRavi ZoreÎncă nu există evaluări
- Heartbeat Irregularities ExplainedDocument5 paginiHeartbeat Irregularities ExplainedKayelyn-Rose Combate100% (1)
- Aortic Stenosis:: Updates in Diagnosis & ManagementDocument48 paginiAortic Stenosis:: Updates in Diagnosis & ManagementCuca PcelaÎncă nu există evaluări
- Focal Atrial Tachycardia I: Clinical Features, DiagnosisDocument10 paginiFocal Atrial Tachycardia I: Clinical Features, Diagnosisapi-26166949Încă nu există evaluări
- PedsnotesDocument18 paginiPedsnoteskp13oyÎncă nu există evaluări
- A Handbook of Multivalvular and Prosthetic Valve DiseaseDe la EverandA Handbook of Multivalvular and Prosthetic Valve DiseaseÎncă nu există evaluări
- Temporary Pacemaker Settings and CareDocument51 paginiTemporary Pacemaker Settings and Carewaqas_xsÎncă nu există evaluări
- Ecg Pathology 02Document95 paginiEcg Pathology 02Andi MP Manurung100% (1)
- RV (Dys)function assessment by echocardiographyDocument52 paginiRV (Dys)function assessment by echocardiographyNag Mallesh RaoÎncă nu există evaluări
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- EKG Clep TestDocument13 paginiEKG Clep TestElissa LafondÎncă nu există evaluări
- Narasimha EngDocument33 paginiNarasimha EngSachin SinghÎncă nu există evaluări
- All Ventricular Muscle Cells Beat at The Same Time BecauseDocument25 paginiAll Ventricular Muscle Cells Beat at The Same Time Becauseliyana04_08Încă nu există evaluări
- L-R ShuntDocument88 paginiL-R ShuntnanohaniwiekoÎncă nu există evaluări
- Aortopulmonary Window Repair at Seoul National University HospitalDocument13 paginiAortopulmonary Window Repair at Seoul National University HospitalHugo GonzálezÎncă nu există evaluări
- Echocardiographic Evaluation of Prosthetic Heart ValvesDocument64 paginiEchocardiographic Evaluation of Prosthetic Heart ValvesNavojit ChowdhuryÎncă nu există evaluări
- A Handbook On Clinical Echo CardiographyDocument71 paginiA Handbook On Clinical Echo Cardiographysri RamalakshmiÎncă nu există evaluări
- CARDIOLOGYDocument4 paginiCARDIOLOGYJeewaka Prebashwara DayarathneÎncă nu există evaluări
- Heart Failure Express Card HMCDocument2 paginiHeart Failure Express Card HMCalexÎncă nu există evaluări
- Cardiac SarcoidosisDocument13 paginiCardiac SarcoidosisEmeric Jorge Macedo VendezuÎncă nu există evaluări
- Mechanisms of Cardiac Arrhythmias From Automatici+Document24 paginiMechanisms of Cardiac Arrhythmias From Automatici+Malar MannanÎncă nu există evaluări
- Braunwald Lecture Series #2Document33 paginiBraunwald Lecture Series #2usfcards100% (2)
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 paginiChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoÎncă nu există evaluări
- CHAPTER 55 - Percutaneous Coronary InterventionDocument1 paginăCHAPTER 55 - Percutaneous Coronary InterventionReda SoÎncă nu există evaluări
- Ward Reflection PaperDocument1 paginăWard Reflection PaperReda SoÎncă nu există evaluări
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 paginiRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoÎncă nu există evaluări
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 paginiChapter 32 - Genetic Cardiac ArrythmiasReda SoÎncă nu există evaluări
- Tilt Table Testing: Name Age/Sex APDocument1 paginăTilt Table Testing: Name Age/Sex APReda SoÎncă nu există evaluări
- Braunwald Chapter KeypointersDocument6 paginiBraunwald Chapter KeypointersReda SoÎncă nu există evaluări
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 paginiCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoÎncă nu există evaluări
- CH 50 - Approach To Patient With Chest PainDocument1 paginăCH 50 - Approach To Patient With Chest PainReda SoÎncă nu există evaluări
- Name: - Year LevelDocument6 paginiName: - Year LevelReda SoÎncă nu există evaluări
- Answer Key-Mitral ValveDocument6 paginiAnswer Key-Mitral ValveReda SoÎncă nu există evaluări
- Private Ward Admission Census 1Document6 paginiPrivate Ward Admission Census 1Reda SoÎncă nu există evaluări
- CHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Document1 paginăCHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Reda SoÎncă nu există evaluări
- Evidence-Based Approach to Heart Failure History and Physical ExamDocument5 paginiEvidence-Based Approach to Heart Failure History and Physical ExamReda SoÎncă nu există evaluări
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 paginiCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoÎncă nu există evaluări
- Rapid Response and Cardiac Arrest TeamsDocument11 paginiRapid Response and Cardiac Arrest TeamsReda SoÎncă nu există evaluări
- Trials SummaryDocument12 paginiTrials SummaryReda SoÎncă nu există evaluări
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 paginiCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoÎncă nu există evaluări
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 paginiVascular Conference: JUNE 2018 - MARCH 2019Reda SoÎncă nu există evaluări
- Cardiology census and patient detailsDocument9 paginiCardiology census and patient detailsReda SoÎncă nu există evaluări
- Heart Institute Team Building April 2019Document1 paginăHeart Institute Team Building April 2019Reda SoÎncă nu există evaluări
- Marijuana LegalizationDocument5 paginiMarijuana LegalizationMatt ImpellusoÎncă nu există evaluări
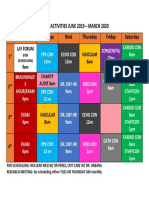
- Daily Activities 2019Document1 paginăDaily Activities 2019Reda SoÎncă nu există evaluări
- Tilt Table Testing: Name Age/Sex APDocument1 paginăTilt Table Testing: Name Age/Sex APReda SoÎncă nu există evaluări
- Computed Tomography Findings for 8 Cardiovascular PatientsDocument1 paginăComputed Tomography Findings for 8 Cardiovascular PatientsReda SoÎncă nu există evaluări
- 2011 PadDocument19 pagini2011 PadReda SoÎncă nu există evaluări
- Case Protocol 3Document5 paginiCase Protocol 3Reda SoÎncă nu există evaluări
- Case Protocol 3Document2 paginiCase Protocol 3Reda SoÎncă nu există evaluări
- Culture of BMWDocument6 paginiCulture of BMWhk246100% (1)
- Ororbia Maze LearningDocument10 paginiOrorbia Maze LearningTom WestÎncă nu există evaluări
- Urban Process Design - Hamid ShirvaniDocument1 paginăUrban Process Design - Hamid ShirvaniCaramel LatteÎncă nu există evaluări
- Bruno Latour: What Is Iconoclash?Document3 paginiBruno Latour: What Is Iconoclash?Clara HabibÎncă nu există evaluări
- Vadiyanatha AstakamDocument4 paginiVadiyanatha AstakamRaga MalikaÎncă nu există evaluări
- Philosophical Perspectives Through the AgesDocument13 paginiPhilosophical Perspectives Through the Agesshashankmay18Încă nu există evaluări
- Role of TaxationDocument5 paginiRole of TaxationCarlo Francis Palma100% (1)
- MF 04Document21 paginiMF 04Carlos De la CruzÎncă nu există evaluări
- Modelling of Induction Motor PDFDocument42 paginiModelling of Induction Motor PDFsureshÎncă nu există evaluări
- Test Unit 3Document2 paginiTest Unit 3RAMONA SECUÎncă nu există evaluări
- German composer known for political worksDocument4 paginiGerman composer known for political worksGeorge PikÎncă nu există evaluări
- Librarianship and Professional Ethics: Understanding Standards for Library ProfessionalsDocument12 paginiLibrarianship and Professional Ethics: Understanding Standards for Library ProfessionalsHALLÎncă nu există evaluări
- Why Research Is Important in The BusinessDocument2 paginiWhy Research Is Important in The BusinessBricx BalerosÎncă nu există evaluări
- Neoclassicism: Romanticism Realism ImpressionismDocument16 paginiNeoclassicism: Romanticism Realism ImpressionismErika EludoÎncă nu există evaluări
- Neandertal Birth Canal Shape and The Evo PDFDocument6 paginiNeandertal Birth Canal Shape and The Evo PDFashkenadaharsaÎncă nu există evaluări
- ISE I Conversation Task - Rules and RegulationsDocument3 paginiISE I Conversation Task - Rules and RegulationsElena B. HerreroÎncă nu există evaluări
- BSC Part IiDocument76 paginiBSC Part IiAbhi SinghÎncă nu există evaluări
- ASBMR 14 Onsite Program Book FINALDocument362 paginiASBMR 14 Onsite Program Book FINALm419703Încă nu există evaluări
- The Meaning of Al FatihaDocument11 paginiThe Meaning of Al Fatihammhoward20Încă nu există evaluări
- Tle-Bpp 8-Q1-M18Document14 paginiTle-Bpp 8-Q1-M18Michelle LlanesÎncă nu există evaluări
- CBCP Monitor Vol. 17 No. 9Document20 paginiCBCP Monitor Vol. 17 No. 9Areopagus Communications, Inc.Încă nu există evaluări
- Distance Learning 2016 Telecom AcademyDocument17 paginiDistance Learning 2016 Telecom AcademyDyego FelixÎncă nu există evaluări
- Merry Almost Christmas - A Year With Frog and Toad (Harmonies)Document6 paginiMerry Almost Christmas - A Year With Frog and Toad (Harmonies)gmit92Încă nu există evaluări
- Umair Mazher ThesisDocument44 paginiUmair Mazher Thesisumair_mazherÎncă nu există evaluări
- The Role of Christian Education in Socia Group 6Document6 paginiThe Role of Christian Education in Socia Group 6Ṭhanuama BiateÎncă nu există evaluări