S-ar putea să vă placă și
- Bsped Dka Guideline 2020Document24 paginiBsped Dka Guideline 2020Valentina Jiménez CárdenasÎncă nu există evaluări
- Dka GuidelinesDocument24 paginiDka GuidelinesVeena GawaliÎncă nu există evaluări
- Guidelines For The Management of Diabetic Ketoacidosis (DKA) in AdultsDocument21 paginiGuidelines For The Management of Diabetic Ketoacidosis (DKA) in AdultsCristina BadarauÎncă nu există evaluări
- Guideline For The Management of Children and Young People Under The Age of 18 Years With Diabetic Ketoacidosis (DKA)Document26 paginiGuideline For The Management of Children and Young People Under The Age of 18 Years With Diabetic Ketoacidosis (DKA)Arslan SiddiquiÎncă nu există evaluări
- Dka GuidelineDocument16 paginiDka GuidelineGhada HusseinÎncă nu există evaluări
- Johns Hopkins DKA Clinical PathwayDocument31 paginiJohns Hopkins DKA Clinical PathwayPatricia Denise Tome MagisaÎncă nu există evaluări
- Management of Diabetic Ketoacidosis: A Summary of The 2013 Joint British Diabetes Societies GuidelinesDocument4 paginiManagement of Diabetic Ketoacidosis: A Summary of The 2013 Joint British Diabetes Societies GuidelinesErik Jaya GunawanÎncă nu există evaluări
- Pediatric Diabetes - 2022 - GlaserDocument22 paginiPediatric Diabetes - 2022 - GlasersyukriÎncă nu există evaluări
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 paginiDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheFelipe GaribayÎncă nu există evaluări
- Management of Diabetic Ketoacidosis: MW SavageDocument3 paginiManagement of Diabetic Ketoacidosis: MW SavagedramaysinghÎncă nu există evaluări
- Guia 13481Document22 paginiGuia 13481CarmenÎncă nu există evaluări
- Cetoacidosis 2022Document20 paginiCetoacidosis 2022David RojasÎncă nu există evaluări
- Abrir Cetoacidosis 2022Document20 paginiAbrir Cetoacidosis 2022Giovanny Alexander BravoÎncă nu există evaluări
- Guia Ispad 2022 Cetoacidosis Diabetica y Estadi HiperosmolarDocument22 paginiGuia Ispad 2022 Cetoacidosis Diabetica y Estadi HiperosmolarElizabeth Cross50% (2)
- Dka & HHS - Ispad 2022Document16 paginiDka & HHS - Ispad 2022Bladimir CentenoÎncă nu există evaluări
- Ispad - Pediatric DiabetesDocument22 paginiIspad - Pediatric Diabetesfernandovenega313Încă nu există evaluări
- Diabetic Ketoacidosis (DKA) : BackgroundDocument9 paginiDiabetic Ketoacidosis (DKA) : Backgroundalyssa_flores_3Încă nu există evaluări
- Diabetic Medicine 2022 The Management of Diabetic KetoacidosisDocument20 paginiDiabetic Medicine 2022 The Management of Diabetic KetoacidosisasmÎncă nu există evaluări
- EM CRIT CETOACIDOSIS LLLDocument18 paginiEM CRIT CETOACIDOSIS LLLGiovannaÎncă nu există evaluări
- Final Corrected DKA AselaDocument32 paginiFinal Corrected DKA AselaabelÎncă nu există evaluări
- Diabetes National Clinical Guidelines For The Management of Diabetic KetoacidosisDocument17 paginiDiabetes National Clinical Guidelines For The Management of Diabetic KetoacidosisSean EdwardsÎncă nu există evaluări
- Management of Diabetic Ketoacidosis: MW SavageDocument3 paginiManagement of Diabetic Ketoacidosis: MW SavageChristian SalimÎncă nu există evaluări
- Metabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSDocument5 paginiMetabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSMahmoud khedrÎncă nu există evaluări
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 paginiDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheCynthia SarmientoÎncă nu există evaluări
- Paediatric DKA Integrated Care Pathway For CportalDocument39 paginiPaediatric DKA Integrated Care Pathway For Cportalteresita vargasÎncă nu există evaluări
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 paginiPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaÎncă nu există evaluări
- Seminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Document34 paginiSeminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Meraol HusseinÎncă nu există evaluări
- BDC Dka Treatment Protocol 2018 85Document12 paginiBDC Dka Treatment Protocol 2018 85MohammedÎncă nu există evaluări
- Diabetic Ketoacidosis PathwayDocument22 paginiDiabetic Ketoacidosis PathwaySri Nath100% (1)
- The Management of Diabetic Ketoacidosis in Adults-An Updated GuidelineDocument20 paginiThe Management of Diabetic Ketoacidosis in Adults-An Updated GuidelineDudu FrechianiÎncă nu există evaluări
- Diabetic KetoacidosisDocument10 paginiDiabetic Ketoacidosisagar agarÎncă nu există evaluări
- Diabetic Emergencies - 2011 - Katsilambros - Multiple Choice QuestionsDocument14 paginiDiabetic Emergencies - 2011 - Katsilambros - Multiple Choice QuestionsRyan ReÎncă nu există evaluări
- Arterial Blood Gas (Abg)Document10 paginiArterial Blood Gas (Abg)Kita kitaÎncă nu există evaluări
- Fluid Management in MalnutritionDocument30 paginiFluid Management in MalnutritionCHALIE MEQUÎncă nu există evaluări
- Complicaciones en DiabetesDocument10 paginiComplicaciones en DiabetesJhaann Franco UPÎncă nu există evaluări
- Tatalaksana Kad 1Document7 paginiTatalaksana Kad 1Nurul Kamilah SadliÎncă nu există evaluări
- Practical Guide To Inpatient Glycaemic Care - V2 2020Document115 paginiPractical Guide To Inpatient Glycaemic Care - V2 2020shahirahÎncă nu există evaluări
- 1 Insulin Infusion Responses inDocument6 pagini1 Insulin Infusion Responses inPedro Henrique SoaresÎncă nu există evaluări
- Dka ThesisDocument5 paginiDka Thesissow1vosanyv3100% (2)
- PBL DiscussionsDocument70 paginiPBL DiscussionsMaria ThereseÎncă nu există evaluări
- CS Diabetic KetoacidosisDocument11 paginiCS Diabetic KetoacidosisMarvin Dela CruzÎncă nu există evaluări
- Guidelines For Management of Diabetic Ketoacidosis. Time To ReviseDocument3 paginiGuidelines For Management of Diabetic Ketoacidosis. Time To ReviseeduÎncă nu există evaluări
- Dr. ComatDocument11 paginiDr. ComatDarwin SantiagoÎncă nu există evaluări
- Updates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCDocument7 paginiUpdates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCLenin Zavaleta RodriguezÎncă nu există evaluări
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 paginiDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From Thenguyenngocanh9798Încă nu există evaluări
- Guideline Title: Management of Diabetic KetoacidosisDocument9 paginiGuideline Title: Management of Diabetic KetoacidosisJorge Salazar GomezÎncă nu există evaluări
- ISPAD Covid &DKADocument9 paginiISPAD Covid &DKAkermi inesseÎncă nu există evaluări
- Diabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheDocument20 paginiDiabetic Medicine - 2022 - Dhatariya - The Management of Diabetic Ketoacidosis in Adults An Updated Guideline From TheEman HendyÎncă nu există evaluări
- A K N H: Evidence Based Clinical Practice Guidelines For The Management of Pediatric DKADocument16 paginiA K N H: Evidence Based Clinical Practice Guidelines For The Management of Pediatric DKAAL AHLIÎncă nu există evaluări
- Emergency Diabetes 2023 - Septian Mixrova SebayangDocument30 paginiEmergency Diabetes 2023 - Septian Mixrova SebayangFiqri DzulfaqqorÎncă nu există evaluări
- Endocrine Emergencies in PicuDocument10 paginiEndocrine Emergencies in PicuDr.MohanÎncă nu există evaluări
- Diabetic Ketoacidosis (DKA)Document33 paginiDiabetic Ketoacidosis (DKA)Eric Chye Teck100% (1)
- 2018 IspadDocument28 pagini2018 IspadJohana JuarezÎncă nu există evaluări
- Emergency Management of Diabetic Ketoacidosis in Adults: ReviewDocument5 paginiEmergency Management of Diabetic Ketoacidosis in Adults: ReviewRenisa HutahaeanÎncă nu există evaluări
- IJPRDocument6 paginiIJPRUlvi DitasariÎncă nu există evaluări
- Midterms LecDocument276 paginiMidterms LecmyÎncă nu există evaluări
- CC EP 126 Diabetes Mellitus and Disorders of Glucose Homeostasis Ch. 118 Rosens 9th Ed. 1Document13 paginiCC EP 126 Diabetes Mellitus and Disorders of Glucose Homeostasis Ch. 118 Rosens 9th Ed. 1Ikenna EzeiloÎncă nu există evaluări
- Closing The Gap: DKA Management PearlsDocument12 paginiClosing The Gap: DKA Management PearlsSyed Shahrul Naz SyedÎncă nu există evaluări
- Diabetes NCLEX QuestionsDocument22 paginiDiabetes NCLEX QuestionsGesta, Van Gerard T.Încă nu există evaluări
- An Approach To Paediatric Abdominal PainDocument32 paginiAn Approach To Paediatric Abdominal PaindrsaleemÎncă nu există evaluări
- Rationale For Consideration of Statins For COVID 19 PatientDocument7 paginiRationale For Consideration of Statins For COVID 19 PatientdrsaleemÎncă nu există evaluări
- Paediatric Diabetes Care: SPIN Module Curriculum inDocument36 paginiPaediatric Diabetes Care: SPIN Module Curriculum indrsaleemÎncă nu există evaluări
- 1503Document810 pagini1503Miguel Santos100% (1)
- Ada PDFDocument204 paginiAda PDFMario BarbozaÎncă nu există evaluări
- Paediatric Diabetes Care: SPIN Module Curriculum inDocument36 paginiPaediatric Diabetes Care: SPIN Module Curriculum indrsaleemÎncă nu există evaluări
- Hematuria in PediatricsDocument4 paginiHematuria in PediatricsKousik AmancharlaÎncă nu există evaluări
- Risk Factors For Severe COVID 19Document3 paginiRisk Factors For Severe COVID 19drsaleemÎncă nu există evaluări
- Haematuria: Definition / Supporting InformationDocument8 paginiHaematuria: Definition / Supporting InformationdrsaleemÎncă nu există evaluări
- Friends-Not-Masters-A Political Autobiography By-President Ayub-Khan PDFDocument263 paginiFriends-Not-Masters-A Political Autobiography By-President Ayub-Khan PDFHaider razaÎncă nu există evaluări
- (The Pelican Guide To English Literature, Vol. 6) Boris Ford-The Pelican Guide To English Literature 6 - From Dickens To Hardy-Penguin BooksDocument524 pagini(The Pelican Guide To English Literature, Vol. 6) Boris Ford-The Pelican Guide To English Literature 6 - From Dickens To Hardy-Penguin Booksdrsaleem92% (13)
- Diabetes & Clinic Organisation ENGDocument28 paginiDiabetes & Clinic Organisation ENGdrsaleemÎncă nu există evaluări
- 5000 Three Forms of English Verbs With Urdu MeaningDocument153 pagini5000 Three Forms of English Verbs With Urdu Meaningdrsaleem92% (24)
- Uptdate PediatricsDocument451 paginiUptdate PediatricsdrsaleemÎncă nu există evaluări
- Idiopathic Thrombocytopenic Purpura in Children CA1072 v4Document15 paginiIdiopathic Thrombocytopenic Purpura in Children CA1072 v4drsaleemÎncă nu există evaluări
- English, Third Edition: An Analysis of Longman Dictionary of ContemporaryDocument15 paginiEnglish, Third Edition: An Analysis of Longman Dictionary of ContemporarydrsaleemÎncă nu există evaluări
- Tas 2017.3Document11 paginiTas 2017.3drsaleemÎncă nu există evaluări
- 2011 ITP Pocket Guide PDFDocument4 pagini2011 ITP Pocket Guide PDFWinda AlpiniawatiÎncă nu există evaluări
- CGMDocument10 paginiCGMdrsaleemÎncă nu există evaluări
- Coping With Diabetes ENGDocument24 paginiCoping With Diabetes ENGdrsaleemÎncă nu există evaluări
- Diabetes and The Growing Child ENGDocument30 paginiDiabetes and The Growing Child ENGdrsaleemÎncă nu există evaluări
- Diabetes and The Growing Child ENGDocument30 paginiDiabetes and The Growing Child ENGdrsaleemÎncă nu există evaluări
- Diabetes and Routine Care ENGDocument39 paginiDiabetes and Routine Care ENGdrsaleemÎncă nu există evaluări
- Diabetes and Chronic Care Plan ENGDocument24 paginiDiabetes and Chronic Care Plan ENGdrsaleemÎncă nu există evaluări
- 3b. Emergency Care - Hypoglycaemia ENGDocument15 pagini3b. Emergency Care - Hypoglycaemia ENGdrsaleemÎncă nu există evaluări
- 3c. Emergency Care - Surgery ENGDocument15 pagini3c. Emergency Care - Surgery ENGdrsaleemÎncă nu există evaluări
- Practical Medical Procedures at A GlanceDocument10 paginiPractical Medical Procedures at A GlancedrsaleemÎncă nu există evaluări
- 3a Emergency Care DKA (UK) FINALDocument40 pagini3a Emergency Care DKA (UK) FINALDrsarfaraz SiddiquiÎncă nu există evaluări
- Diagnosing Diabetes ENGDocument25 paginiDiagnosing Diabetes ENGdrsaleemÎncă nu există evaluări
- Value-Based Care Metrics: Blood PressureDocument2 paginiValue-Based Care Metrics: Blood PressureDorios TorresÎncă nu există evaluări
- How Is Type 2 Diabetes Treated - What To Know If You Are Newly DiagnosedDocument2 paginiHow Is Type 2 Diabetes Treated - What To Know If You Are Newly DiagnosedRatnaPrasadNalamÎncă nu există evaluări
- Counseling The Newly Diabetic Patient FinalDocument33 paginiCounseling The Newly Diabetic Patient Finalapi-546809761Încă nu există evaluări
- 3-Yoga As Preventive Measures For Lifestyle DiseasesDocument22 pagini3-Yoga As Preventive Measures For Lifestyle DiseasesDivyanshu YadavÎncă nu există evaluări
- Impact of Yoga On Diabetes MillitusDocument8 paginiImpact of Yoga On Diabetes MillitusMurthy0% (1)
- 1 s2.0 S168719792100040X MainDocument4 pagini1 s2.0 S168719792100040X MainfelipetheÎncă nu există evaluări
- Prieto Stiffany 4B g4 Pt4-Week-5Document10 paginiPrieto Stiffany 4B g4 Pt4-Week-5Stiffany PrietoÎncă nu există evaluări
- AC Final Research DEFENDED CutieeeDocument156 paginiAC Final Research DEFENDED CutieeeKim Razon SemblanteÎncă nu există evaluări
- Hemmingsen Et Al-2017-Cochrane Database of Systematic ReviewsDocument192 paginiHemmingsen Et Al-2017-Cochrane Database of Systematic ReviewsUfiq MantoÎncă nu există evaluări
- 2014-JNC-8-Hypertension WRDocument2 pagini2014-JNC-8-Hypertension WRismailuntung0% (1)
- SGLT2 Inhibitors and MechanismsDocument7 paginiSGLT2 Inhibitors and MechanismseswaynedÎncă nu există evaluări
- E Book Advance Training On Medical Nutrition Part-IDocument74 paginiE Book Advance Training On Medical Nutrition Part-IMohammadEhtashamÎncă nu există evaluări
- Clinical Management of DiabetesDocument13 paginiClinical Management of DiabetesMark TallyÎncă nu există evaluări
- حالات سكرDocument13 paginiحالات سكرNada AliÎncă nu există evaluări
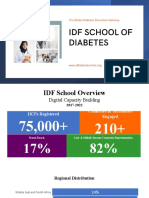
- IDF School - Overview - Oct 2022 - HMS - Prof - EnriqueDocument29 paginiIDF School - Overview - Oct 2022 - HMS - Prof - EnriquesameerÎncă nu există evaluări
- NCP HypomagnesemiaDocument2 paginiNCP HypomagnesemiaMark Zedrix MediarioÎncă nu există evaluări
- JBDS 11 Management of Adults With Diabetes On Dialysis Summary of Recommendations September 2022Document26 paginiJBDS 11 Management of Adults With Diabetes On Dialysis Summary of Recommendations September 2022AchrafÎncă nu există evaluări
- Manajemen DM Tipe 2 - HBD Idi LabuselDocument40 paginiManajemen DM Tipe 2 - HBD Idi LabuselJunni EdyÎncă nu există evaluări
- Poverty Increases Type 2 Diabetes Incidence and Inequality of Care Despite Universal Health CoverageDocument7 paginiPoverty Increases Type 2 Diabetes Incidence and Inequality of Care Despite Universal Health CoverageHitmanÎncă nu există evaluări
- Fdocuments - in - PHD Progress ReportDocument35 paginiFdocuments - in - PHD Progress ReportYASSER ALDEOESÎncă nu există evaluări
- Exercise and Type 2 DiabetesDocument15 paginiExercise and Type 2 Diabetespb.nakulaÎncă nu există evaluări
- Health Literacy, Illness Perception, Depression, and Selfmanagement Among African Americans With Type 2 DiabetesDocument9 paginiHealth Literacy, Illness Perception, Depression, and Selfmanagement Among African Americans With Type 2 Diabetesloshaana105Încă nu există evaluări
- Diabetes Mellitus OSCEDocument11 paginiDiabetes Mellitus OSCEjoryadelmÎncă nu există evaluări
- Subcutaneous Injection: Humalog U-100 or U-200: More CommonDocument2 paginiSubcutaneous Injection: Humalog U-100 or U-200: More Commonahmad ryanÎncă nu există evaluări
- Case Simulation 119Document3 paginiCase Simulation 119Alexis Sebastian DionisioÎncă nu există evaluări
- Diabetes Problem Based Learning PDFDocument6 paginiDiabetes Problem Based Learning PDFIfantri Pramana100% (1)
- Cause and EffectDocument16 paginiCause and EffectMJ CORPUZÎncă nu există evaluări
- Obesity Management As A Primary Treatment Goal For Type 2 DiabetesDocument12 paginiObesity Management As A Primary Treatment Goal For Type 2 DiabetesGonzalo Francisco Miranda ManriqueÎncă nu există evaluări
- PROPOTION OF TYPE 2 DIABETES MELLITUS PATIENTS WITH INTEGRATED USE OF ALLOPATHIC AND INDIAN SYSTEM OF MEDICINE AND ITS BENEFITS AND SIDE EFFECTS AMONG ADULTS ABOVE 40 YR FOR DM IN SOUTH KERALA India new-converted.pdfDocument14 paginiPROPOTION OF TYPE 2 DIABETES MELLITUS PATIENTS WITH INTEGRATED USE OF ALLOPATHIC AND INDIAN SYSTEM OF MEDICINE AND ITS BENEFITS AND SIDE EFFECTS AMONG ADULTS ABOVE 40 YR FOR DM IN SOUTH KERALA India new-converted.pdfAfladul MubeenppÎncă nu există evaluări
- Mogensen 1983Document15 paginiMogensen 1983Mădălina MitroiuÎncă nu există evaluări