S-ar putea să vă placă și
- Nonclinical Safety Assessment: A Guide to International Pharmaceutical RegulationsDe la EverandNonclinical Safety Assessment: A Guide to International Pharmaceutical RegulationsWilliam J. BrockÎncă nu există evaluări
- Portfolio, Program, and Project Management in the Pharmaceutical and Biotechnology IndustriesDe la EverandPortfolio, Program, and Project Management in the Pharmaceutical and Biotechnology IndustriesPete HarpumÎncă nu există evaluări
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewDe la EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewÎncă nu există evaluări
- Social Aspects of Drug Discovery, Development and CommercializationDe la EverandSocial Aspects of Drug Discovery, Development and CommercializationÎncă nu există evaluări
- Real-World Evidence in the Pharmaceutical LandscapeDe la EverandReal-World Evidence in the Pharmaceutical LandscapeÎncă nu există evaluări
- Oral Controlled Release Formulation Design and Drug Delivery: Theory to PracticeDe la EverandOral Controlled Release Formulation Design and Drug Delivery: Theory to PracticeHong WenÎncă nu există evaluări
- Multivariate Analysis in the Pharmaceutical IndustryDe la EverandMultivariate Analysis in the Pharmaceutical IndustryAna Patricia FerreiraÎncă nu există evaluări
- Inhaled Pharmaceutical Product Development Perspectives: Challenges and OpportunitiesDe la EverandInhaled Pharmaceutical Product Development Perspectives: Challenges and OpportunitiesÎncă nu există evaluări
- Cost-Contained Regulatory Compliance: For the Pharmaceutical, Biologics, and Medical Device IndustriesDe la EverandCost-Contained Regulatory Compliance: For the Pharmaceutical, Biologics, and Medical Device IndustriesÎncă nu există evaluări
- Protocol Template 05feb2016 508Document3 paginiProtocol Template 05feb2016 508Dwi Annisa AmaliaSariÎncă nu există evaluări
- EVALUATING CLINICAL Studies of Antimicrobials in The Division of Antiinfective Drug ProductsDocument102 paginiEVALUATING CLINICAL Studies of Antimicrobials in The Division of Antiinfective Drug ProductsMichael wang100% (1)
- Clinical Guidelines Ecbs 2001Document52 paginiClinical Guidelines Ecbs 2001Ajay KumarÎncă nu există evaluări
- Defining Your Target Product Profile Therapeutics Workbook TemplateDocument8 paginiDefining Your Target Product Profile Therapeutics Workbook TemplateaamiralichauhanÎncă nu există evaluări
- Protocol Template - Early Phase.2Document36 paginiProtocol Template - Early Phase.2Vasiliy KÎncă nu există evaluări
- Medical Devices Proposal For A Regulation - 2012 - 542 - enDocument194 paginiMedical Devices Proposal For A Regulation - 2012 - 542 - enRoxanaBurlaÎncă nu există evaluări
- RAPS Online U CatalogDocument22 paginiRAPS Online U CatalogvinayÎncă nu există evaluări
- FDA Regulation of Medical DevicesDocument40 paginiFDA Regulation of Medical DevicesAyub NaveedÎncă nu există evaluări
- 06 PSUR PBRER Thomas MunzDocument35 pagini06 PSUR PBRER Thomas MunzMohabKamalÎncă nu există evaluări
- Guide To Clinical Trial Protocol Content and FormatDocument8 paginiGuide To Clinical Trial Protocol Content and FormatRohit Manakchand ZawarÎncă nu există evaluări
- Clinical Trials Data ManagementDocument3 paginiClinical Trials Data ManagementAyush JainÎncă nu există evaluări
- Schedule YDocument30 paginiSchedule Yapi-3810976100% (13)
- Key Concepts of Clinical Trials A Narrative ReviewDocument12 paginiKey Concepts of Clinical Trials A Narrative ReviewLaura CampañaÎncă nu există evaluări
- CGMP in Clinical InvestigationDocument44 paginiCGMP in Clinical InvestigationrwbbartonÎncă nu există evaluări
- Ind Studies by Sejal KhumanDocument34 paginiInd Studies by Sejal KhumanSejal khumamÎncă nu există evaluări
- Early Development Best Practices For Stability-Regulatory PerspectiveDocument20 paginiEarly Development Best Practices For Stability-Regulatory PerspectiveMartin CelestinoÎncă nu există evaluări
- Overview of Drug Discovery and Development ProcessesDocument17 paginiOverview of Drug Discovery and Development ProcessesMelissa STanÎncă nu există evaluări
- RUSSIAN DRUG REGISTRATION CHANGESDocument9 paginiRUSSIAN DRUG REGISTRATION CHANGESashwanÎncă nu există evaluări
- Critical AppraisalDocument6 paginiCritical AppraisalLudi Dhyani RahmartaniÎncă nu există evaluări
- Clinicaltrials Presentation 111011025509 Phpapp02 PDFDocument51 paginiClinicaltrials Presentation 111011025509 Phpapp02 PDFGayathri Parthasarathy100% (1)
- GSK b2c109575 Clinical Study Report Redact PDFDocument1.524 paginiGSK b2c109575 Clinical Study Report Redact PDFdhananjayÎncă nu există evaluări
- CTD and eCTDDocument5 paginiCTD and eCTDSri harsha reddyÎncă nu există evaluări
- Complexities of Medical Device TestingDocument2 paginiComplexities of Medical Device TestingKeri Gobin SamarooÎncă nu există evaluări
- Understanding Clinical TrialsDocument56 paginiUnderstanding Clinical Trialspharma000Încă nu există evaluări
- Quality by Design A Present To Future PerspectiveDocument8 paginiQuality by Design A Present To Future PerspectiveEditor IJTSRDÎncă nu există evaluări
- RWE Update: Collecting Real-World Healthcare DataDocument10 paginiRWE Update: Collecting Real-World Healthcare DataHananAhmedÎncă nu există evaluări
- Clinical Trial PhasesDocument11 paginiClinical Trial Phasesheyyo ggÎncă nu există evaluări
- FDA Guidance PMS and Clinical TrialsDocument21 paginiFDA Guidance PMS and Clinical TrialsJonna SapiterÎncă nu există evaluări
- An Overview of The US Regulatory System For OTC ProductsDocument6 paginiAn Overview of The US Regulatory System For OTC Productsanimeluis100% (1)
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 paginiSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- SITE GEN-001 01 - SOP On Site ActivitiesDocument17 paginiSITE GEN-001 01 - SOP On Site ActivitiesCR Professionals IndiaÎncă nu există evaluări
- Experimental Design in Clinical TrialsDocument18 paginiExperimental Design in Clinical Trialsarun_azamÎncă nu există evaluări
- Clinical Trial DesignsDocument18 paginiClinical Trial DesignsVenkatesh Gavini100% (1)
- NEWS CENTER Maine (NCM) Sent A List of Questions To The FDA and These Were Their ResponsesDocument2 paginiNEWS CENTER Maine (NCM) Sent A List of Questions To The FDA and These Were Their ResponsesNEWS CENTER MaineÎncă nu există evaluări
- CTD Modules PDFDocument5 paginiCTD Modules PDFsrideviÎncă nu există evaluări
- Site FDA inspection checklistDocument9 paginiSite FDA inspection checklistsreeraj.guruvayoorÎncă nu există evaluări
- Understanding Clinical Trials: Developed by Sara Back, NP Bronx-Lebanon Hospital CenterDocument41 paginiUnderstanding Clinical Trials: Developed by Sara Back, NP Bronx-Lebanon Hospital Centeranubha_naikÎncă nu există evaluări
- Auditing: Clinical Research StudiesDocument7 paginiAuditing: Clinical Research StudiesRenzo FernandezÎncă nu există evaluări
- Abnormal Returns and Cash Flows in Pharmaceutical M&A PDFDocument61 paginiAbnormal Returns and Cash Flows in Pharmaceutical M&A PDFJoachim_91Încă nu există evaluări
- Biocompatibility Protocols for Medical Devices and MaterialsDe la EverandBiocompatibility Protocols for Medical Devices and MaterialsÎncă nu există evaluări
- An Introduction to Clinical Trials: Design Issues and Study TypesDocument29 paginiAn Introduction to Clinical Trials: Design Issues and Study TypesJay BingoÎncă nu există evaluări
- Clinical Research AssociateDocument2 paginiClinical Research AssociatepalkybdÎncă nu există evaluări
- Automated Signal DetectionDocument7 paginiAutomated Signal DetectionSutirtho MukherjiÎncă nu există evaluări
- Site FDA Prep CklistDocument15 paginiSite FDA Prep Cklistana.acreis100% (2)
- Protocol Designing in CTDocument5 paginiProtocol Designing in CTSushma Reddy VÎncă nu există evaluări
- Works For Sanofi AventisDocument6 paginiWorks For Sanofi AventisMohit AroraÎncă nu există evaluări
- Principles and Practice of Clinical TrialsDocument2.573 paginiPrinciples and Practice of Clinical TrialsZuriÎncă nu există evaluări
- Clinical Trial Transparency (TranspariMED 2017) 20171212Document40 paginiClinical Trial Transparency (TranspariMED 2017) 20171212Till BrucknerÎncă nu există evaluări
- Drug Discovery and Development HandoutDocument5 paginiDrug Discovery and Development HandoutGermie PosionÎncă nu există evaluări
- CMCDocument3 paginiCMCSri harsha reddyÎncă nu există evaluări
- Laporan Pemakaian Dan Lembar Permintaan Obat (Lplpo) PuskesmasDocument7 paginiLaporan Pemakaian Dan Lembar Permintaan Obat (Lplpo) PuskesmasNoviana Kurnia AmbarwatiÎncă nu există evaluări
- Maccoy Stika DrugsDocument4 paginiMaccoy Stika Drugsapi-445856719Încă nu există evaluări
- Midterm Exam PCT LecDocument5 paginiMidterm Exam PCT LecRichard OcampoÎncă nu există evaluări
- Monitoring Penggunaan Obat Generik di Rumah Sakit Ciputra HospitalDocument15 paginiMonitoring Penggunaan Obat Generik di Rumah Sakit Ciputra HospitalMujiyanto RichardÎncă nu există evaluări
- شرح HPLC 2Document138 paginiشرح HPLC 2radyomarelqadyÎncă nu există evaluări
- Drug StudyDocument2 paginiDrug Studykurunot juntillaÎncă nu există evaluări
- Non LINIER FARMAKOKINETIK (Tinjauan Dari Segi Klinik)Document12 paginiNon LINIER FARMAKOKINETIK (Tinjauan Dari Segi Klinik)Dian GabriellaÎncă nu există evaluări
- Data Farklin Apt. Faizal 27 Maret-18 April PDFDocument27 paginiData Farklin Apt. Faizal 27 Maret-18 April PDFfarklin rsuamiraÎncă nu există evaluări
- AmayuDocument1 paginăAmayuPranoy MayuriÎncă nu există evaluări
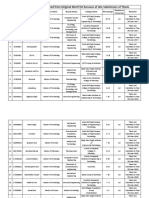
- Students Removed from Merit List Due to Late Thesis SubmissionDocument2 paginiStudents Removed from Merit List Due to Late Thesis SubmissionDivyanshu AggarwalÎncă nu există evaluări
- Common Disk-Shaped Tablets A Tablet Is A Mixture of ActiveDocument8 paginiCommon Disk-Shaped Tablets A Tablet Is A Mixture of Activenasser9876Încă nu există evaluări
- Regulatory Trends Tighten Rules on Cross-Contamination in Drug ManufacturingDocument9 paginiRegulatory Trends Tighten Rules on Cross-Contamination in Drug Manufacturinglina kharratÎncă nu există evaluări
- PharmacologyDocument21 paginiPharmacologyMaridel Estioco100% (3)
- Medisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25DDocument2 paginiMedisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25Dhk_scribdÎncă nu există evaluări
- Metoclopramide - WikipediaDocument25 paginiMetoclopramide - WikipediaMuhammadafif SholehuddinÎncă nu există evaluări
- Introduction to Pharmacokinetics: Basic ConceptsDocument7 paginiIntroduction to Pharmacokinetics: Basic ConceptsJeraldiin BeltranÎncă nu există evaluări
- Pharmacologic management of adult breakthrough cancer painDocument4 paginiPharmacologic management of adult breakthrough cancer painousama aklan100% (1)
- Pricing Reimbursement Drugs In: IndiaDocument28 paginiPricing Reimbursement Drugs In: IndiaGiang HoàngÎncă nu există evaluări
- PERCOBAAN I FARMAKOKINETIK RevisiDocument9 paginiPERCOBAAN I FARMAKOKINETIK RevisiYustinÎncă nu există evaluări
- Principles of Drug ActionDocument42 paginiPrinciples of Drug ActionsharmamtechÎncă nu există evaluări
- CV ScoleDocument3 paginiCV Scoleapi-609125382Încă nu există evaluări
- PHARMACOLOGYDocument9 paginiPHARMACOLOGYapi-198635480% (1)
- Ribociclib: Protocol Ref: Mpharibobr (Version No: 1.1)Document10 paginiRibociclib: Protocol Ref: Mpharibobr (Version No: 1.1)Joana JohnÎncă nu există evaluări
- 10.1.2 - Antacid Agents (2007-Jan2016)Document14 pagini10.1.2 - Antacid Agents (2007-Jan2016)Gabrielle NnomoÎncă nu există evaluări
- Restricted Drugs and Non FormularyDocument2 paginiRestricted Drugs and Non FormularyChristine Joy De OcampoÎncă nu există evaluări
- Pharma Trans Le1Document60 paginiPharma Trans Le1Kunal TribhuvanÎncă nu există evaluări
- The Role of The Pharmacist in The Health Care SystemDocument6 paginiThe Role of The Pharmacist in The Health Care SystemZain AlviÎncă nu există evaluări
- MD Final Year Rasa Shashtra and Bhishaja Kalpana 151114 PDFDocument14 paginiMD Final Year Rasa Shashtra and Bhishaja Kalpana 151114 PDFBhavana GangurdeÎncă nu există evaluări
- Affordable medicines and medical suppliesDocument12 paginiAffordable medicines and medical suppliesTrie Gusti linglingÎncă nu există evaluări
- Folic Acid Drug StudyDocument1 paginăFolic Acid Drug Studysha rcÎncă nu există evaluări