S-ar putea să vă placă și
- Hary-Fluid Management Part 1Document49 paginiHary-Fluid Management Part 1Keta PatelÎncă nu există evaluări
- Intravenous Fluid Therapy in Adults in The HospitalDocument28 paginiIntravenous Fluid Therapy in Adults in The Hospitalushapadminivadivelswamy100% (2)
- Fluid ManagementDocument10 paginiFluid ManagementdradaadÎncă nu există evaluări
- Parenteral Fluid TherapyDocument5 paginiParenteral Fluid TherapyAbdalrahman KhalilÎncă nu există evaluări
- Management Dengue HXDocument6 paginiManagement Dengue HXMalshika JayatissaÎncă nu există evaluări
- Fluid GuidelinesDocument8 paginiFluid GuidelinesAya SalahÎncă nu există evaluări
- IvfDocument17 paginiIvfBima BaikuniÎncă nu există evaluări
- DehydrationDocument10 paginiDehydrationAbdelrahman M. AlnweiriÎncă nu există evaluări
- Fluid Management in Neonates and InfantsDocument51 paginiFluid Management in Neonates and InfantsSulabh Shrestha100% (1)
- Fluid and Electrolyte NewDocument54 paginiFluid and Electrolyte NewSelam Tesfaye ShebaÎncă nu există evaluări
- Guideline, Management of HypernatremiaDocument9 paginiGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- Guidance For Intravenous Fluid and Electrolyte Prescription in AdultsDocument8 paginiGuidance For Intravenous Fluid and Electrolyte Prescription in AdultsfrakturhepatikaÎncă nu există evaluări
- Manajemen Perioperatif Terapi Cairan Pada PediatriDocument35 paginiManajemen Perioperatif Terapi Cairan Pada PediatriZulhendraÎncă nu există evaluări
- DKA Protocol TGDocument11 paginiDKA Protocol TGabelÎncă nu există evaluări
- Acute Renal Failure (Diagnosis Approach and ManagementDocument24 paginiAcute Renal Failure (Diagnosis Approach and ManagementPrasad RauÎncă nu există evaluări
- Surgery YbDocument67 paginiSurgery YbTamirat geletaÎncă nu există evaluări
- Principles+ +LU6Document35 paginiPrinciples+ +LU6Alvin Ray JuanÎncă nu există evaluări
- Fluid and ElectrolytesDocument179 paginiFluid and ElectrolytesTrixie Al Marie75% (4)
- Dr. Faiez Alhmoud Albashir Teaching HospitalDocument76 paginiDr. Faiez Alhmoud Albashir Teaching HospitalDr-Firas Nayf Al-ThawabiaÎncă nu există evaluări
- Fluid & Electrolytes in SurgeryDocument64 paginiFluid & Electrolytes in SurgeryakunmereclarkÎncă nu există evaluări
- Fluid and Electrolyte TherapyDocument39 paginiFluid and Electrolyte TherapyrikarzÎncă nu există evaluări
- 2017 Fluid and Electrolytes LECTURE NOTESDocument34 pagini2017 Fluid and Electrolytes LECTURE NOTESHarley Justiniani Dela CruzÎncă nu există evaluări
- 19 Fluid and Electrolyte Imbalance and Nutritional ProblemDocument40 pagini19 Fluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerÎncă nu există evaluări
- Fluid Calculation For Iv InfusionDocument8 paginiFluid Calculation For Iv InfusionAsma SaleemÎncă nu există evaluări
- Fluid and Electrolyte Therapy - SeblewongelDocument47 paginiFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeÎncă nu există evaluări
- IV Fluid TherapyDocument28 paginiIV Fluid TherapyJacinta MaryÎncă nu există evaluări
- Endocrine Emergencies in PicuDocument10 paginiEndocrine Emergencies in PicuDr.MohanÎncă nu există evaluări
- Fluid and Electrolytes: Ma. Medine L. Amorsolo RN ManDocument29 paginiFluid and Electrolytes: Ma. Medine L. Amorsolo RN ManMichael Baylon Dueñas100% (1)
- Maintenance Fluid Therapy in ChildrenDocument4 paginiMaintenance Fluid Therapy in ChildrenNicole_0Încă nu există evaluări
- Fluid and Electrolyte Management of Surgical Patient PDFDocument37 paginiFluid and Electrolyte Management of Surgical Patient PDFJie CuetoÎncă nu există evaluări
- Body FluidDocument37 paginiBody FluidBir Mohammad SonetÎncă nu există evaluări
- Fluids&LytesDocument33 paginiFluids&LytesMateen ShukriÎncă nu există evaluări
- Maintenance Intravenous Fluid Therapy in Children - UpToDateDocument19 paginiMaintenance Intravenous Fluid Therapy in Children - UpToDaterolland_arrizaÎncă nu există evaluări
- IV Fluid TherapyDocument28 paginiIV Fluid Therapyansuh2250% (2)
- Pedia Alhamdollilah FluidsDocument80 paginiPedia Alhamdollilah FluidsArwyn AncogÎncă nu există evaluări
- Perioperative Fluid Management in ChildrenDocument31 paginiPerioperative Fluid Management in ChildrenRashmi SahaÎncă nu există evaluări
- Fluid & Electrolytes SaurabhDocument88 paginiFluid & Electrolytes Saurabhunknownsince1986Încă nu există evaluări
- Dehydration: Body-Fluid CompositionDocument5 paginiDehydration: Body-Fluid CompositionThegreat Mokz Mokz ThegreatÎncă nu există evaluări
- Fluid and Electrolytes.3Document43 paginiFluid and Electrolytes.3Medic PediatruÎncă nu există evaluări
- Under The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsDocument63 paginiUnder The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsHenley AndrewsÎncă nu există evaluări
- Pediatric Fluid and Electrolyte TherapyDocument27 paginiPediatric Fluid and Electrolyte TherapyNanda Cendikia100% (1)
- IvfDocument16 paginiIvfJohnRev Fundal Lopez LorenzoÎncă nu există evaluări
- Fluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju AshokanDocument31 paginiFluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju Ashokanvaishnavi kaleÎncă nu există evaluări
- Fluid Replacement TherapyDocument3 paginiFluid Replacement TherapyJesusreignsÎncă nu există evaluări
- 1 FluidsDocument17 pagini1 FluidsMae CalunsagÎncă nu există evaluări
- DKADocument5 paginiDKAMariel BernabeÎncă nu există evaluări
- Diabetes Insipidus.Document10 paginiDiabetes Insipidus.Nithya ManiÎncă nu există evaluări
- Case 1a Answer KeyDocument4 paginiCase 1a Answer KeyChettan Kerala100% (1)
- Tests of Tubular FunctionDocument4 paginiTests of Tubular FunctionDr-Dalya ShakirÎncă nu există evaluări
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 paginiAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Fluids and ElectrolyteDocument25 paginiFluids and Electrolytehammadkhan7126Încă nu există evaluări
- Hypernatremia: Marielle Adey R. Magcawas BSN-3CDocument28 paginiHypernatremia: Marielle Adey R. Magcawas BSN-3CMarielle Adey Magcawas RNÎncă nu există evaluări
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDocument23 paginiDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- Acute Kidney InjuryDocument43 paginiAcute Kidney InjuryIwan ToniroÎncă nu există evaluări
- Roumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistDocument59 paginiRoumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistYenyen DelgadoÎncă nu există evaluări
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDocument34 paginiFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?De la EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?Încă nu există evaluări
- Solutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeDe la EverandSolutions to Diabetes and Hypoglycemia (Translated): How to prevent and get rid of it in a natural way, without resorting to medicines but adopting a correct way of lifeÎncă nu există evaluări
- Ovarian and Fallopian Tube PathologyDocument5 paginiOvarian and Fallopian Tube PathologyShelley PantinopleÎncă nu există evaluări
- Ob Gyn PDFDocument29 paginiOb Gyn PDFShelley PantinopleÎncă nu există evaluări
- CASE PRES (Cholecystitis)Document132 paginiCASE PRES (Cholecystitis)Shelley PantinopleÎncă nu există evaluări
- Pe Pedia - KeyDocument83 paginiPe Pedia - KeyShelley PantinopleÎncă nu există evaluări
- Kwento Ni Rosario Reaction PaperDocument4 paginiKwento Ni Rosario Reaction PaperShelley Pantinople67% (3)
- Physiology Review - Cellular, Hematopoesis, HemostasisDocument33 paginiPhysiology Review - Cellular, Hematopoesis, HemostasisShelley PantinopleÎncă nu există evaluări
- 3a1 Batch Review - Physiology 2Document239 pagini3a1 Batch Review - Physiology 2Shelley Pantinople100% (1)
- A Vision of Heaven and Eternity - Prepare For The Lords Return by Bernada FernandezDocument9 paginiA Vision of Heaven and Eternity - Prepare For The Lords Return by Bernada FernandezGeorgeStoneEsq3100% (3)
- COVID GuidelinesDocument54 paginiCOVID GuidelinesHBÎncă nu există evaluări
- Final Update On Antenatal Steroids - DR PadmeshDocument66 paginiFinal Update On Antenatal Steroids - DR PadmeshAhalia NicuÎncă nu există evaluări
- Home Study Course-HomeopathDocument155 paginiHome Study Course-HomeopathAzad Ansari67% (6)
- DEPRESSANTSDocument18 paginiDEPRESSANTSElisha Arwynne Postrero RomaÎncă nu există evaluări
- 01-2020 - Tactical Emergency Casualty Care (TECC)Document5 pagini01-2020 - Tactical Emergency Casualty Care (TECC)pibulinÎncă nu există evaluări
- Pediatric Medication AdministrationDocument59 paginiPediatric Medication AdministrationHilary Alvarado100% (1)
- Lecture 3 PsychopharmacologyDocument99 paginiLecture 3 PsychopharmacologyPavan chowdaryÎncă nu există evaluări
- E-Health & Its BenifitsDocument19 paginiE-Health & Its BenifitsKomal HiraveÎncă nu există evaluări
- Borrelia RecurrentisDocument10 paginiBorrelia RecurrentisSamJavi65Încă nu există evaluări
- Blood CirculationDocument42 paginiBlood CirculationAshu kumar100% (1)
- Aga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsDocument15 paginiAga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsRamzan BibiÎncă nu există evaluări
- Investigatory Project On AnalgesicsDocument30 paginiInvestigatory Project On AnalgesicsAnurag Singh100% (1)
- Oncology Scope of ServicesDocument2 paginiOncology Scope of ServicesJaisurya SharmaÎncă nu există evaluări
- Clinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsDocument2 paginiClinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsChantal CarnesÎncă nu există evaluări
- S Tahel 2005Document12 paginiS Tahel 2005Catherine MorrisÎncă nu există evaluări
- BiologyDocument14 paginiBiologyKanish KumarÎncă nu există evaluări
- 15 English PPT Nursing 5 ADocument208 pagini15 English PPT Nursing 5 ASinta WuLandari100% (1)
- Autoimmune Rheumatic DiseasesDocument3 paginiAutoimmune Rheumatic DiseasesBuat DownloadÎncă nu există evaluări
- Hospitalization and Its Effect For Patient - UNTAD 2011 PDFDocument26 paginiHospitalization and Its Effect For Patient - UNTAD 2011 PDFRiris SutrisnoÎncă nu există evaluări
- Regenerative Medicine From Protocol To PatientDocument257 paginiRegenerative Medicine From Protocol To PatientMandraludinÎncă nu există evaluări
- Nursing Care Plans - Nursing Dia - Gulanick, MegDocument1.374 paginiNursing Care Plans - Nursing Dia - Gulanick, Megeric parl91% (22)
- Aron FinalDocument70 paginiAron FinalJaime Pastrana Jr.Încă nu există evaluări
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocument7 paginiManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaÎncă nu există evaluări
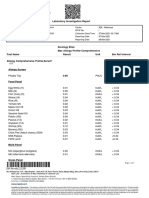
- Laboratory Investigation ReportDocument7 paginiLaboratory Investigation ReportAmarjeetÎncă nu există evaluări
- The Cracked Mirror, Karen KernbergDocument10 paginiThe Cracked Mirror, Karen Kernbergjuaromer100% (1)
- Research Paper - Stem Cells-3Document11 paginiResearch Paper - Stem Cells-3api-549248786Încă nu există evaluări
- Law Exam NotesDocument11 paginiLaw Exam NotesEric Cheng100% (1)
- Bochdalek Hernia - Wikipedia, The Free Encyclopedia PDFDocument5 paginiBochdalek Hernia - Wikipedia, The Free Encyclopedia PDFMilda InayahÎncă nu există evaluări
- Blaylock Forced0415 130Document13 paginiBlaylock Forced0415 130RAMO STEF SZEKERESÎncă nu există evaluări
- Animal Aloksan PDFDocument14 paginiAnimal Aloksan PDFTrias Ilmi PramudikaÎncă nu există evaluări
- Grade 6 PSW Yearend Question PaperDocument8 paginiGrade 6 PSW Yearend Question PaperJerome Buchler100% (1)