S-ar putea să vă placă și
- A CBCT Evaluation of Root Position in Bone, Long Axis Inclination and Relationship To The WALA Ridge - ClinicalKeyDocument20 paginiA CBCT Evaluation of Root Position in Bone, Long Axis Inclination and Relationship To The WALA Ridge - ClinicalKeyKATHERINE JOHANA PEÑA SUAREZÎncă nu există evaluări
- 14 Kelly 1977 Centric Relation, Centric Occlusion, and Posterior Tooth Forms and ArrangementDocument7 pagini14 Kelly 1977 Centric Relation, Centric Occlusion, and Posterior Tooth Forms and Arrangementjorefe12Încă nu există evaluări
- Longitudinal Evaluation of Dental ArchesDocument10 paginiLongitudinal Evaluation of Dental ArchessauriuaÎncă nu există evaluări
- The Monoplane Occlusion For Complete Dentures: T H e SP Herical TheoryDocument7 paginiThe Monoplane Occlusion For Complete Dentures: T H e SP Herical TheorySahana RangarajanÎncă nu există evaluări
- Development of The Curve of SpeeDocument9 paginiDevelopment of The Curve of SpeeMirnaLizÎncă nu există evaluări
- Curve of Spee 2018Document7 paginiCurve of Spee 2018Thendral DevanathanÎncă nu există evaluări
- Redefining Tweed's Headplate Correction and Its Implications in Dental Arch Space RequirementDocument4 paginiRedefining Tweed's Headplate Correction and Its Implications in Dental Arch Space RequirementKanchit SuwanswadÎncă nu există evaluări
- Understanding Anchorage in Orthodontics-Review ArticlesDocument5 paginiUnderstanding Anchorage in Orthodontics-Review ArticlesSoe San KyawÎncă nu există evaluări
- Sorensen Martinioff 1984 Intracoronal and Cuspal Coverage Restorations in EndoDocument5 paginiSorensen Martinioff 1984 Intracoronal and Cuspal Coverage Restorations in EndoKarloz Meza BlancoÎncă nu există evaluări
- Rapid Maxillary Expansion With SkeletalDocument4 paginiRapid Maxillary Expansion With SkeletalDaniela CastilloÎncă nu există evaluări
- Journal of Pharmacy & Bioallied Sciences: Significance of Curve of Spee: An Orthodontic ReviewDocument14 paginiJournal of Pharmacy & Bioallied Sciences: Significance of Curve of Spee: An Orthodontic ReviewAly OsmanÎncă nu există evaluări
- Centric and Eccentric OcclusionsDocument8 paginiCentric and Eccentric OcclusionsYan Lau100% (1)
- Ellinger 1971Document7 paginiEllinger 1971Mohammed TarekÎncă nu există evaluări
- 5 Record Bases & Occlusion RimsDocument36 pagini5 Record Bases & Occlusion RimssabreennafiyaÎncă nu există evaluări
- Biological Guides To The Positioning of The Artificial Teeth in Complete DenturesDocument4 paginiBiological Guides To The Positioning of The Artificial Teeth in Complete DenturesDan Beznoiu100% (2)
- Etiology of Supernumerary Teeth A Literature ReviewDocument6 paginiEtiology of Supernumerary Teeth A Literature ReviewfrvkuhrifÎncă nu există evaluări
- Stone Age Mans Dentition3 Ajo1954Document14 paginiStone Age Mans Dentition3 Ajo1954BeniyaÎncă nu există evaluări
- Excellence in Finishing - Modifications For The Perio-Restorative PatientDocument20 paginiExcellence in Finishing - Modifications For The Perio-Restorative Patientjonathanza14Încă nu există evaluări
- Criteria For Restorable Endo Teetg - CDA-ADC JournalDocument9 paginiCriteria For Restorable Endo Teetg - CDA-ADC Journalmoji_puiÎncă nu există evaluări
- Development of The Curve of SpeeDocument10 paginiDevelopment of The Curve of SpeePratiwi Dwi HartantiÎncă nu există evaluări
- Occlusion, Malocclusion and Method of Measurements - An OverviewDocument7 paginiOcclusion, Malocclusion and Method of Measurements - An OverviewDiana BernardÎncă nu există evaluări
- Single Complete DentureDocument26 paginiSingle Complete Denturedrsoumyapromod75% (8)
- Evaluation Abutment Tooth:: Prof. Adel Farhan IbraheemDocument12 paginiEvaluation Abutment Tooth:: Prof. Adel Farhan IbraheemMohammad AÎncă nu există evaluări
- Occlusion in Implant DentistryDocument9 paginiOcclusion in Implant DentistrydrsmritiÎncă nu există evaluări
- ABO Grading SystemDocument82 paginiABO Grading Systemsanjeed sanjuÎncă nu există evaluări
- Una Clasificacion de Los Fenotipos Oseos Crestales Dentoalveolares RadicularesDocument9 paginiUna Clasificacion de Los Fenotipos Oseos Crestales Dentoalveolares RadicularesZulma Moreno HuertasÎncă nu există evaluări
- JCDP 19 624Document4 paginiJCDP 19 624Priyanka GandhiÎncă nu există evaluări
- 1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneDocument35 pagini1947 Howes CASE ANALYSIS AND TREATMENT PLANNING BASED UPON THE Relationship of Tooth Material To Its Supporting BoneRockey ShrivastavaÎncă nu există evaluări
- Curve of SpeeDocument7 paginiCurve of SpeeKorina CallerosÎncă nu există evaluări
- Occlusion As Reked To Co Prosthodontics Refrtow E: Complete DenturesDocument11 paginiOcclusion As Reked To Co Prosthodontics Refrtow E: Complete DenturesKrupali JainÎncă nu există evaluări
- Occlusal Concepts in Complete Denture Prosthodontics: A Literature ReviewDocument5 paginiOcclusal Concepts in Complete Denture Prosthodontics: A Literature ReviewSahana RangarajanÎncă nu există evaluări
- The Single Complete Denture - A Case Report: Usha M Radke, Sham M Gundawar, Rajlakshmi S Banarjee, Aditi S PaldiwalDocument6 paginiThe Single Complete Denture - A Case Report: Usha M Radke, Sham M Gundawar, Rajlakshmi S Banarjee, Aditi S Paldiwaljinan AlanaziÎncă nu există evaluări
- 3 Single CDDocument7 pagini3 Single CDdrgayen6042Încă nu există evaluări
- Single Complete Denture FinalDocument15 paginiSingle Complete Denture FinalVikas AggarwalÎncă nu există evaluări
- Becker Bone Anatomy Interdental RegionDocument6 paginiBecker Bone Anatomy Interdental RegionDr. DeeptiÎncă nu există evaluări
- Serial Extractions - A Review PDFDocument8 paginiSerial Extractions - A Review PDFJose CollazosÎncă nu există evaluări
- Retention and RelapseDocument97 paginiRetention and RelapseModit Gupta75% (4)
- Dimension VerticalDocument17 paginiDimension Verticalger moralesÎncă nu există evaluări
- Occlusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsDocument16 paginiOcclusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsHector Flores Soto100% (4)
- Stone Age Mans Dentition1 Ajo1954Document15 paginiStone Age Mans Dentition1 Ajo1954BeniyaÎncă nu există evaluări
- Concept of Shortened Dental Arch An OverviewDocument3 paginiConcept of Shortened Dental Arch An OverviewHarold CamargoÎncă nu există evaluări
- Extracciones Seriadas 15Document8 paginiExtracciones Seriadas 15Mirita AliauÎncă nu există evaluări
- Concepts of Arrangement of Artifical Teeth, SelectiveDocument7 paginiConcepts of Arrangement of Artifical Teeth, SelectiveAmar BhochhibhoyaÎncă nu există evaluări
- Biomechanical Considerations in Restoring Endodontically Treated Teeth-Assif1994Document3 paginiBiomechanical Considerations in Restoring Endodontically Treated Teeth-Assif1994Dan MPÎncă nu există evaluări
- AnchorageDocument52 paginiAnchorageharshiniÎncă nu există evaluări
- J of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsDocument6 paginiJ of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsManuel CastilloÎncă nu există evaluări
- J of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsDocument6 paginiJ of Oral Rehabilitation - 2021 - Zonnenberg - Centric Relation Critically Revisited What Are The Clinical ImplicationsVasu SinghÎncă nu există evaluări
- Finishing & Detailing in OrthodonticsDocument16 paginiFinishing & Detailing in OrthodonticsBikramjeet Singh71% (7)
- FPD - LEC.SAS.8 Chart Factors Influencing Bridge DesignDocument11 paginiFPD - LEC.SAS.8 Chart Factors Influencing Bridge DesignabegailnalzaroÎncă nu există evaluări
- Complete Dentures: Bone Resorption and ProsthodonticsDocument7 paginiComplete Dentures: Bone Resorption and ProsthodonticsPriyanka GandhiÎncă nu există evaluări
- Serial ExtDocument12 paginiSerial Extrahul sharmaÎncă nu există evaluări
- Full Mouth ReconstructDocument5 paginiFull Mouth ReconstructMuaiyed Buzayan AkremyÎncă nu există evaluări
- Assignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'Document19 paginiAssignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'nivitha naidu100% (1)
- Article 1525968342 PDFDocument10 paginiArticle 1525968342 PDFanindhitha thandapaniÎncă nu există evaluări
- Balanced Occlusion: Dr. Rakshith HegdeDocument104 paginiBalanced Occlusion: Dr. Rakshith HegdePragya Jain67% (3)
- Gainsforth 1945Document12 paginiGainsforth 1945Víctor Adolfo Ravelo SalinasÎncă nu există evaluări
- Evolution of Dental Tissues and Paleobiology in SelachiansDe la EverandEvolution of Dental Tissues and Paleobiology in SelachiansÎncă nu există evaluări
- Long 'on' the Tooth: Dental Evidence of DietDe la EverandLong 'on' the Tooth: Dental Evidence of DietÎncă nu există evaluări
- Biomechanics in Lingual Orthodontics What The Fut - 2018 - Seminars in Orthodon PDFDocument9 paginiBiomechanics in Lingual Orthodontics What The Fut - 2018 - Seminars in Orthodon PDFOmy J. CruzÎncă nu există evaluări
- Evaluating The Accuracy of Facial Models Obtained From Vol - 2018 - Seminars in PDFDocument8 paginiEvaluating The Accuracy of Facial Models Obtained From Vol - 2018 - Seminars in PDFOmy J. CruzÎncă nu există evaluări
- Lingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDFDocument15 paginiLingual Orthodontics Understanding The Issues Is The Ke - 2018 - Seminars in or PDFOmy J. CruzÎncă nu există evaluări
- 3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFDocument7 pagini3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFOmy J. CruzÎncă nu există evaluări
- Accuracy of Digital Predictions With CAD CAM Labial and L - 2018 - Seminars in O PDFDocument14 paginiAccuracy of Digital Predictions With CAD CAM Labial and L - 2018 - Seminars in O PDFOmy J. CruzÎncă nu există evaluări
- Clinical Guidelines For Direct Printed Metal Orthodo - 2018 - Seminars in Orthod PDFDocument9 paginiClinical Guidelines For Direct Printed Metal Orthodo - 2018 - Seminars in Orthod PDFOmy J. CruzÎncă nu există evaluări
- Diagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFDocument8 paginiDiagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFOmy J. CruzÎncă nu există evaluări
- Introduction 2019 Seminars-in-OrthodonticsDocument2 paginiIntroduction 2019 Seminars-in-OrthodonticsOmy J. CruzÎncă nu există evaluări
- Comparison of Traditional RPE With Two Types of Micro I - 2019 - Seminars in OrtDocument9 paginiComparison of Traditional RPE With Two Types of Micro I - 2019 - Seminars in OrtOmy J. Cruz100% (1)
- Adult Transverse Diagnosis and Treatment A Case Ba - 2019 - Seminars in OrthodoDocument40 paginiAdult Transverse Diagnosis and Treatment A Case Ba - 2019 - Seminars in OrthodoOmy J. Cruz100% (1)
- Chem Resist ChartDocument13 paginiChem Resist ChartRC LandaÎncă nu există evaluări
- Agile ModelingDocument15 paginiAgile Modelingprasad19845Încă nu există evaluări
- P. E. and Health ReportDocument20 paginiP. E. and Health ReportLESSLY ABRENCILLOÎncă nu există evaluări
- Redirection & PipingDocument16 paginiRedirection & PipingPraveen PatelÎncă nu există evaluări
- Invoices For UEG IstanbulDocument7 paginiInvoices For UEG IstanbulIesaw IesawÎncă nu există evaluări
- Manual Ares-G2 2Document78 paginiManual Ares-G2 2CarolDiasÎncă nu există evaluări
- Practical Cs Xii Mysql 2022-23 FinalDocument9 paginiPractical Cs Xii Mysql 2022-23 FinalHimanshu GuptaÎncă nu există evaluări
- Eng21 (Story of Hamguchi Gohei)Document9 paginiEng21 (Story of Hamguchi Gohei)Alapan NandaÎncă nu există evaluări
- Obara BogbeDocument36 paginiObara BogbeOjubona Aremu Omotiayebi Ifamoriyo0% (1)
- AstmDocument5 paginiAstmyanurarzaqaÎncă nu există evaluări
- A SURVEY OF ENVIRONMENTAL REQUIREMENTS FOR THE MIDGE (Diptera: Tendipedidae)Document15 paginiA SURVEY OF ENVIRONMENTAL REQUIREMENTS FOR THE MIDGE (Diptera: Tendipedidae)Batuhan ElçinÎncă nu există evaluări
- ICD10WHO2007 TnI4Document1.656 paginiICD10WHO2007 TnI4Kanok SongprapaiÎncă nu există evaluări
- De DusterDocument6 paginiDe DusterArstÎncă nu există evaluări
- Functions: Var S AddDocument13 paginiFunctions: Var S AddRevati MenghaniÎncă nu există evaluări
- Assignment Csi104Document11 paginiAssignment Csi104Minh Lê KhảiÎncă nu există evaluări
- Optimal Dispatch of Generation: Prepared To Dr. Emaad SedeekDocument7 paginiOptimal Dispatch of Generation: Prepared To Dr. Emaad SedeekAhmedRaafatÎncă nu există evaluări
- TrellisDocument1 paginăTrellisCayenne LightenÎncă nu există evaluări
- BECIL Registration Portal: How To ApplyDocument2 paginiBECIL Registration Portal: How To ApplySoul BeatsÎncă nu există evaluări
- Model TB-16Document20 paginiModel TB-16xuanphuong2710Încă nu există evaluări
- 0 BA Design ENDocument12 pagini0 BA Design ENFilho AiltonÎncă nu există evaluări
- 2013 Cases Penned by Justice BernabeDocument11 pagini2013 Cases Penned by Justice BernabeJoan PabloÎncă nu există evaluări
- Asus Test ReportDocument4 paginiAsus Test ReportFerry RiantoÎncă nu există evaluări
- Hydrogeological Survey and Eia Tor - Karuri BoreholeDocument3 paginiHydrogeological Survey and Eia Tor - Karuri BoreholeMutonga Kitheko100% (1)
- Bachelors - Harvest Moon Animal ParadeDocument12 paginiBachelors - Harvest Moon Animal ParaderikaÎncă nu există evaluări
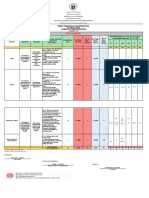
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Document6 paginiRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoÎncă nu există evaluări
- Better Photography - April 2018 PDFDocument100 paginiBetter Photography - April 2018 PDFPeter100% (1)
- LG Sigma+EscalatorDocument4 paginiLG Sigma+Escalator강민호Încă nu există evaluări
- IPM GuidelinesDocument6 paginiIPM GuidelinesHittesh SolankiÎncă nu există evaluări
- Estate TaxDocument10 paginiEstate TaxCharrie Grace PabloÎncă nu există evaluări
- Bài Tập Từ Loại Ta10Document52 paginiBài Tập Từ Loại Ta10Trinh TrầnÎncă nu există evaluări