S-ar putea să vă placă și
- CBRN Individual Protective Equipment Smart CardDocument2 paginiCBRN Individual Protective Equipment Smart CardJoe BennettÎncă nu există evaluări
- TPR CombinedArmsCWMD TacticalPlanningConsiderations (U) AWG 20160625 PDFDocument2 paginiTPR CombinedArmsCWMD TacticalPlanningConsiderations (U) AWG 20160625 PDFJoe BennettÎncă nu există evaluări
- C-WMD Small Unit Leaders SmartcardDocument2 paginiC-WMD Small Unit Leaders SmartcardJoe BennettÎncă nu există evaluări
- C-WMD Small Unit CBRN Detection Equipment Smart CardDocument2 paginiC-WMD Small Unit CBRN Detection Equipment Smart CardJoe Bennett0% (1)
- Urban Poverty Final Exam-PaperDocument12 paginiUrban Poverty Final Exam-PaperJoe BennettÎncă nu există evaluări
- The Conservation of Angular MomentumDocument5 paginiThe Conservation of Angular MomentumJoe BennettÎncă nu există evaluări
- Immortal Technique ProjectDocument7 paginiImmortal Technique ProjectJoe BennettÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Activity 1Document3 paginiActivity 1Clarin Perez OrdinarioÎncă nu există evaluări
- Effectiveness of Eccentric Exercise in Tennis Elbow - A Single CaseDocument2 paginiEffectiveness of Eccentric Exercise in Tennis Elbow - A Single Caseirfan setiadiÎncă nu există evaluări
- Near Misses: Toolbox Meeting GuideDocument1 paginăNear Misses: Toolbox Meeting GuideIwan MsÎncă nu există evaluări
- Low Frequency QsDocument6 paginiLow Frequency QsRon FranklinÎncă nu există evaluări
- Ankle Foot OrthosesDocument14 paginiAnkle Foot OrthosesRohail Farid OrakzaiÎncă nu există evaluări
- Marrow 5 BlueprintDocument18 paginiMarrow 5 Blueprintthe dheeraj sainiÎncă nu există evaluări
- RCTDocument33 paginiRCTHema Chandra Reddy KarimireddyÎncă nu există evaluări
- NCP Impaired Skin IntegrityDocument2 paginiNCP Impaired Skin Integritysnay axieÎncă nu există evaluări
- (Cruel Reality Series #2) Sinful Affair (Author-Ljmxdxnx)Document215 pagini(Cruel Reality Series #2) Sinful Affair (Author-Ljmxdxnx)jsjisksolsllsÎncă nu există evaluări
- Assault & Battery NoteDocument6 paginiAssault & Battery NoteAmir AkmalÎncă nu există evaluări
- Neet Structural Organisation in Animals Important QuestionsDocument18 paginiNeet Structural Organisation in Animals Important QuestionsARKA NEET BIOLOGYÎncă nu există evaluări
- Module 5 - CwtsDocument23 paginiModule 5 - CwtsJim Carlo ChiongÎncă nu există evaluări
- SISS - Diagnostic Adjuncts During Primary SurveyDocument7 paginiSISS - Diagnostic Adjuncts During Primary SurveyPrincy100% (1)
- Wound 2013 0465Document9 paginiWound 2013 0465AlinaRellyyÎncă nu există evaluări
- Physical Exercises For Preventing Injuries Among Adult Male Football Players: A Systematic ReviewDocument8 paginiPhysical Exercises For Preventing Injuries Among Adult Male Football Players: A Systematic ReviewSara PinheiroÎncă nu există evaluări
- 1.10 ANATOMY - The Eyeball - Surface Anatomy - Landmarks - Extrinsic - Intrinsic MusclesDocument3 pagini1.10 ANATOMY - The Eyeball - Surface Anatomy - Landmarks - Extrinsic - Intrinsic MusclesPaolo NaguitÎncă nu există evaluări
- Muscle Origin Insertion Nerve Supply Nerve Rootsa Action 8 T1Document6 paginiMuscle Origin Insertion Nerve Supply Nerve Rootsa Action 8 T1Joshua AgawinÎncă nu există evaluări
- Fitness Professionals' Guide To Musculoskeletal Anatomy and Human Movement (PDFDrive)Document771 paginiFitness Professionals' Guide To Musculoskeletal Anatomy and Human Movement (PDFDrive)Bryan Huarita100% (2)
- Shoulder Rehabilitation Strategies, Guidelines, and PracticeDocument10 paginiShoulder Rehabilitation Strategies, Guidelines, and PracticeoscarÎncă nu există evaluări
- MOTW Moves From Other Playbooks - GenericDocument5 paginiMOTW Moves From Other Playbooks - GenericmrdanielamonÎncă nu există evaluări
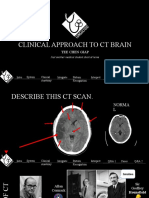
- Clinical Approach To CT BrainDocument34 paginiClinical Approach To CT BrainXiaoThoong LohÎncă nu există evaluări
- People VS GensolaDocument3 paginiPeople VS GensolaLeonardo LawasÎncă nu există evaluări
- Cow SignalsDocument97 paginiCow Signalsblueagave100% (2)
- D435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureDocument73 paginiD435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureD YasIr MussaÎncă nu există evaluări
- FRACTURESDocument1 paginăFRACTURESJAMES PATRICK MONTEMAYORÎncă nu există evaluări
- Ethics Lesson 1Document3 paginiEthics Lesson 1John Lawrence SaatoÎncă nu există evaluări
- Sistema RIADocument36 paginiSistema RIASusan Ly VillalobosÎncă nu există evaluări
- 9th Intra Moot ProblemDocument4 pagini9th Intra Moot Problemmohan kumarÎncă nu există evaluări
- Acetabulum Fractures - Classification and Management - Emile LetournelDocument26 paginiAcetabulum Fractures - Classification and Management - Emile LetournelThanat AuwattanamongkolÎncă nu există evaluări
- Impaired Skin Integrity Related To Surgical Incision and DrainsDocument1 paginăImpaired Skin Integrity Related To Surgical Incision and DrainsGaDis MaNis100% (10)