S-ar putea să vă placă și
- NCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Document1 paginăNCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Shane MedinaÎncă nu există evaluări
- NCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Document1 paginăNCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Gen GenÎncă nu există evaluări
- NCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Document1 paginăNCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Claribel Domingo BayaniÎncă nu există evaluări
- Managing Customer Relationships: Prepare Two Questionnaire's SamplesDocument9 paginiManaging Customer Relationships: Prepare Two Questionnaire's SamplesSana AshrafÎncă nu există evaluări
- Compare NeuroDocument1 paginăCompare Neuroapi-12225640Încă nu există evaluări
- Antipsychotic Pearls Antidepressant Pearls: Class GI Sedating AnticholinergicDocument1 paginăAntipsychotic Pearls Antidepressant Pearls: Class GI Sedating Anticholinergicd_yee90Încă nu există evaluări
- M2C ACTcomparisonchartDocument1 paginăM2C ACTcomparisoncharthow2winÎncă nu există evaluări
- Medical History FormDocument4 paginiMedical History FormHeide Basing-aÎncă nu există evaluări
- MCU PACKAGE PTVI Contractor (Operational Area) SentDocument1 paginăMCU PACKAGE PTVI Contractor (Operational Area) Sentmuh.hasbi asbukÎncă nu există evaluări
- RAHHAL (Risk-Assessment)Document1 paginăRAHHAL (Risk-Assessment)modiÎncă nu există evaluări
- Risk Factor Assessment and Screening and Risk Management: No No No Yes Yes NoDocument1 paginăRisk Factor Assessment and Screening and Risk Management: No No No Yes Yes NomodiÎncă nu există evaluări
- Department of Education: Employee Health and Wellness ProfileDocument1 paginăDepartment of Education: Employee Health and Wellness ProfileGifsy Robledo CastroÎncă nu există evaluări
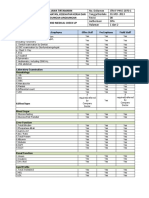
- Pt. Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Standard Medical Check UpDocument2 paginiPt. Jawa Tirtamarin Form Keselamatan, Kesehatan Kerja Dan Perlindungan Lingkungan Standard Medical Check UpWSC IndonesiaÎncă nu există evaluări
- Performance Task #1: A.Directions: Find Different Health Products You Use at Home, Write The Necessary Information AboutDocument4 paginiPerformance Task #1: A.Directions: Find Different Health Products You Use at Home, Write The Necessary Information AboutDYLAN ALESSANDRA FRANCISCOÎncă nu există evaluări
- 1.basics of NutritionDocument23 pagini1.basics of NutritionRaj godhaniyaÎncă nu există evaluări
- Master Data Sheet ActivesDocument1 paginăMaster Data Sheet ActivesKaterina KaradikÎncă nu există evaluări
- Copy of Untitled Form-3vinay - Numbers-Sheet 1-1Document1 paginăCopy of Untitled Form-3vinay - Numbers-Sheet 1-1BvayÎncă nu există evaluări
- Cole Kelby Nutrition Database Form 042018 4Document11 paginiCole Kelby Nutrition Database Form 042018 4api-381003133100% (1)
- Gonek Fitness: Nov 11th Client Bio CardioDocument1 paginăGonek Fitness: Nov 11th Client Bio CardioDanny RomeroÎncă nu există evaluări
- LBLDocument4 paginiLBLKunalSenÎncă nu există evaluări
- Allowed in Nonrestrictive Period Allowed in Restrictive PeriodDocument4 paginiAllowed in Nonrestrictive Period Allowed in Restrictive PeriodEllaÎncă nu există evaluări
- 7.1 Vitamins Basic ConceptsDocument8 pagini7.1 Vitamins Basic Conceptsjpagaran8173Încă nu există evaluări
- Otc Practice Lec 1Document54 paginiOtc Practice Lec 1mahgadÎncă nu există evaluări
- TP Upgrades Thyroid JournalDocument4 paginiTP Upgrades Thyroid JournalgirithaÎncă nu există evaluări
- Optimal Health Blue Print MasterDocument2 paginiOptimal Health Blue Print MastermikidutzaaÎncă nu există evaluări
- Standard Medical Examination FormDocument8 paginiStandard Medical Examination FormritmaratriapÎncă nu există evaluări
- Eating Too Match Yes NoDocument1 paginăEating Too Match Yes NoJonbert AndamÎncă nu există evaluări
- Clinical Pathway NSTEMIDocument2 paginiClinical Pathway NSTEMINurul FitrianaÎncă nu există evaluări
- Bio RevDocument1 paginăBio RevAngel AporÎncă nu există evaluări
- Health Plan: Healthy Mind and Soul A Way of LifeDocument15 paginiHealth Plan: Healthy Mind and Soul A Way of LifePitamber SoniÎncă nu există evaluări
- Ebook VitaminsDocument7 paginiEbook VitaminsRadzÎncă nu există evaluări
- Soap Note 2 Alyssa MatulichDocument8 paginiSoap Note 2 Alyssa Matulichapi-456313554Încă nu există evaluări
- Patient Details: ProblemsDocument4 paginiPatient Details: ProblemsJo GyslingÎncă nu există evaluări
- The Curious Link Between Estrogen and Histamine IntoleranceDocument3 paginiThe Curious Link Between Estrogen and Histamine IntoleranceLika Lanić100% (1)
- Review Cúc: Name Rocher GreenDocument5 paginiReview Cúc: Name Rocher GreenThu HoaiÎncă nu există evaluări
- NutritionalDocument3 paginiNutritionalrashidÎncă nu există evaluări
- Biology ProjectDocument3 paginiBiology ProjectShaik ShaahidÎncă nu există evaluări
- Facility Risk Assessement Form 2016Document1 paginăFacility Risk Assessement Form 2016kojiki67% (3)
- Clinical Pathway STEMIDocument2 paginiClinical Pathway STEMIike rochmadÎncă nu există evaluări
- Fitness Assessment Questionnaire PDFDocument4 paginiFitness Assessment Questionnaire PDFKatrina Pillagara0% (1)
- Healthy Nutritious Food Poster Vegetable and FruiDocument1 paginăHealthy Nutritious Food Poster Vegetable and Fruijssdnl07Încă nu există evaluări
- WedaBay MCU Matrix - Angga SaputraDocument1 paginăWedaBay MCU Matrix - Angga SaputrapelcingÎncă nu există evaluări
- Rekap Stroke RegisterDocument13 paginiRekap Stroke RegisterWulan AzmiÎncă nu există evaluări
- Pharm SimpleNursing PDFDocument192 paginiPharm SimpleNursing PDFDacanay M.A.Încă nu există evaluări
- Lorann 2060 BERGAMOT OIL ALLERGENDocument1 paginăLorann 2060 BERGAMOT OIL ALLERGENVenkat mbaÎncă nu există evaluări
- Penn Smith Skincare Microneedling Protocol 2021Document1 paginăPenn Smith Skincare Microneedling Protocol 2021Mari Morales100% (1)
- Only If Applicable: Please Tick If You Currently or Have Ever Suffered Any of The Following ProblemsDocument3 paginiOnly If Applicable: Please Tick If You Currently or Have Ever Suffered Any of The Following ProblemsLaura ParkaÎncă nu există evaluări
- Coenzima Función de La Coenzima Vitamina Relacionada Función de La Vitamina Fuente de La Vitamina DeficienciaDocument3 paginiCoenzima Función de La Coenzima Vitamina Relacionada Función de La Vitamina Fuente de La Vitamina DeficienciaCristian PulidoÎncă nu există evaluări
- Data Offline Surveilans PTM Berbasis POSBINDU: Tanggal PemeriksaanDocument35 paginiData Offline Surveilans PTM Berbasis POSBINDU: Tanggal PemeriksaanFetty Fatimah Herlina WatiÎncă nu există evaluări
- Lagarto Nutrition in DentistryDocument1 paginăLagarto Nutrition in DentistryVarenLagartoÎncă nu există evaluări
- Gastrointestinal Disorder GIT 2023 - 1Document16 paginiGastrointestinal Disorder GIT 2023 - 1محسن الفهيديÎncă nu există evaluări
- Acidic-: BeneficialDocument112 paginiAcidic-: Beneficialkarthik101Încă nu există evaluări
- Fallowfield Acres Order FormDocument2 paginiFallowfield Acres Order FormJesse PustÎncă nu există evaluări
- D D C Cy Y M M: Client InformationDocument2 paginiD D C Cy Y M M: Client InformationTeressa Wood WrightÎncă nu există evaluări
- 105 DRUGS SOPs FOR YSR CLINICSDocument17 pagini105 DRUGS SOPs FOR YSR CLINICSrajuÎncă nu există evaluări
- COVID-19 Employee Screening Questionnaire GuidelineDocument3 paginiCOVID-19 Employee Screening Questionnaire GuidelinebhaskarÎncă nu există evaluări
- Vitamins and Their Importance - UPSC Guide PDFDocument1 paginăVitamins and Their Importance - UPSC Guide PDFRajesh ManjhiÎncă nu există evaluări
- Clinical MedicineDocument58 paginiClinical Medicinesachin pandaoÎncă nu există evaluări
- Stroke PreventionDocument7 paginiStroke Preventionellla 38Încă nu există evaluări
- Dieta Neoplasm GastricDocument3 paginiDieta Neoplasm Gastricellla 38Încă nu există evaluări
- Psichology of EatingDocument3 paginiPsichology of Eatingellla 38Încă nu există evaluări
- Dynamic Eating Psichology FileDocument1 paginăDynamic Eating Psichology Fileellla 38Încă nu există evaluări
- Pacienta Neoplasm Gastric Operat, 61 Ani. H 167cm, G 40 KG, Activitate Fizica UsoaraDocument2 paginiPacienta Neoplasm Gastric Operat, 61 Ani. H 167cm, G 40 KG, Activitate Fizica Usoaraellla 38Încă nu există evaluări
- The Latest in Cosmetic Medicine Supplements Horm - 2019 - Advances in CosmeticDocument10 paginiThe Latest in Cosmetic Medicine Supplements Horm - 2019 - Advances in Cosmeticellla 38Încă nu există evaluări
- Timing of Food Intake Predicts Weight Loss EffectivenessDocument8 paginiTiming of Food Intake Predicts Weight Loss Effectivenessellla 38Încă nu există evaluări
- Romanian Educational SystemDocument4 paginiRomanian Educational Systemellla 38Încă nu există evaluări
- ReportDocument3 paginiReportellla 38Încă nu există evaluări
- Chocolate: Risk of Heart DiseaseDocument2 paginiChocolate: Risk of Heart Diseaseellla 38Încă nu există evaluări
- Fhs 2450 U4 Essay1Document3 paginiFhs 2450 U4 Essay1api-302132755Încă nu există evaluări
- Chapter One 1.1 DefinitionDocument6 paginiChapter One 1.1 Definitiontsalawa globentÎncă nu există evaluări
- Chapter 91 - Diabetes MellitusDocument75 paginiChapter 91 - Diabetes MellitusPhúc NguyễnÎncă nu există evaluări
- GI TrackDocument125 paginiGI TrackAndika HÎncă nu există evaluări
- 5Document14 pagini5ρενα μινορεÎncă nu există evaluări
- David Perlmutter Full Length InterviewDocument28 paginiDavid Perlmutter Full Length InterviewKalÎncă nu există evaluări
- Euglycemic Diabetic KetoacidosisDocument6 paginiEuglycemic Diabetic KetoacidosisMuhammad BilalÎncă nu există evaluări
- Arid Agriculture University, Rawalpindi: Final Exam / FALL-2020 (Paper Duration 24 Hours) To Be Filled by TeacherDocument10 paginiArid Agriculture University, Rawalpindi: Final Exam / FALL-2020 (Paper Duration 24 Hours) To Be Filled by Teachersaran gul100% (1)
- Bi Kertas 2 Set 2Document23 paginiBi Kertas 2 Set 2Azman Bin JaehÎncă nu există evaluări
- BIO 100 Discoveries in Biology Lecture:09 Autoimmune DisordersDocument29 paginiBIO 100 Discoveries in Biology Lecture:09 Autoimmune DisordersIsmail Hossen RajuÎncă nu există evaluări
- Autoimmune Disorders - AgungDocument40 paginiAutoimmune Disorders - AgungalgutÎncă nu există evaluări
- Rosario - New DataDocument36 paginiRosario - New DataEunice RosarioÎncă nu există evaluări
- Akil Palanisamy MD The TIGER Protocol An Integrative 5 Step Program To Treat and Heal Your AutoimmDocument457 paginiAkil Palanisamy MD The TIGER Protocol An Integrative 5 Step Program To Treat and Heal Your Autoimmharabor madalina100% (1)
- ResearchDocument117 paginiResearchRajeev NepalÎncă nu există evaluări
- Ati Endocrine 2016 1Document6 paginiAti Endocrine 2016 1Jamil AhmedÎncă nu există evaluări
- Continuing Medical Education Akreditasi Idi - 3 SKP Tata Laksana Diabetes Melitus Saat Puasa RamadhanDocument7 paginiContinuing Medical Education Akreditasi Idi - 3 SKP Tata Laksana Diabetes Melitus Saat Puasa RamadhanEstmar ValentinoÎncă nu există evaluări
- Effectiveness of Diabetic Education Programme On The Hba1C Levels Among Type1 Diabetic Children in Omdurman Paediatric HospitalDocument6 paginiEffectiveness of Diabetic Education Programme On The Hba1C Levels Among Type1 Diabetic Children in Omdurman Paediatric HospitalDerison MarsinovaÎncă nu există evaluări
- 239.mudassar DIABETES, PMDC 3811 PAID, Bushra 4011 Not PaidDocument8 pagini239.mudassar DIABETES, PMDC 3811 PAID, Bushra 4011 Not PaidraychandwpÎncă nu există evaluări
- PMP Pathway-9 May 2016Document36 paginiPMP Pathway-9 May 2016Steven LauataÎncă nu există evaluări
- Ismail's Undergraduate ThesisDocument82 paginiIsmail's Undergraduate ThesisAbiola IbrahimÎncă nu există evaluări
- Review About Facts of Diabetes PDFDocument12 paginiReview About Facts of Diabetes PDFmifÎncă nu există evaluări
- Diabetes Mellitus, Diabetes Insipidus and Diabetic Ketoacidosis in ChildrenDocument62 paginiDiabetes Mellitus, Diabetes Insipidus and Diabetic Ketoacidosis in ChildrenGie GenoÎncă nu există evaluări
- (Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mgDocument10 pagini(Product Name) MR Tablet 30mg (Product Name) MR Tablet 60mggmsanto7Încă nu există evaluări
- Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesDocument7 paginiDiabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesReyhan AristoÎncă nu există evaluări
- Bidens Pilosa LDocument40 paginiBidens Pilosa LTia MonikaÎncă nu există evaluări
- Team Approach With Diabetes Patients: HistoryDocument6 paginiTeam Approach With Diabetes Patients: HistoryEdgar SchultzÎncă nu există evaluări
- Mock 3R - Verbal - QDocument7 paginiMock 3R - Verbal - QCherry Grace Articulo DabuconÎncă nu există evaluări
- Nursing Management of Diabetes Mellitus: by Richard A. GuthrieDocument2 paginiNursing Management of Diabetes Mellitus: by Richard A. GuthrieStella GašparušÎncă nu există evaluări
- Senior Project Research PaperDocument16 paginiSenior Project Research Paperapi-309345535100% (1)
- Long COVID19 Syndrome ADocument19 paginiLong COVID19 Syndrome Arbatjun576Încă nu există evaluări