S-ar putea să vă placă și
- Treatment Planning Single Maxillary Anterior Implants for DentistsDe la EverandTreatment Planning Single Maxillary Anterior Implants for DentistsÎncă nu există evaluări
- 2013 Direct Anterior Composites A Practical GuideDocument16 pagini2013 Direct Anterior Composites A Practical Guidemaroun ghalebÎncă nu există evaluări
- Additive Contour of Porcelain Veneers A Key Element in Enamel PreservationDocument13 paginiAdditive Contour of Porcelain Veneers A Key Element in Enamel PreservationPablo BenitezÎncă nu există evaluări
- Denu 2017 44 9 821Document7 paginiDenu 2017 44 9 821Yolanda EvansÎncă nu există evaluări
- Micro and Macro Dental Esthetics: The Key To Smile IndividualizationDocument14 paginiMicro and Macro Dental Esthetics: The Key To Smile IndividualizationRoo GaunaÎncă nu există evaluări
- Direct Posterior Composite Restorations. FinalDocument8 paginiDirect Posterior Composite Restorations. FinalJana AliÎncă nu există evaluări
- BoptloiDocument14 paginiBoptloiSonea M100% (1)
- Advantages of Adhesive in DentistryDocument29 paginiAdvantages of Adhesive in DentistryAnonymous CY62A9Încă nu există evaluări
- 3M ESPE 2013 06 Styleitaliano F EBUDocument11 pagini3M ESPE 2013 06 Styleitaliano F EBUVika KoksÎncă nu există evaluări
- Teflon Tape TechniqueDocument6 paginiTeflon Tape TechniqueJuan K. J. Shin100% (1)
- GRUPO 3 - 2021c - Effective Protocol For Daily High-Quality Direct Posterior Composite Restorations - Layering and FinishingDocument18 paginiGRUPO 3 - 2021c - Effective Protocol For Daily High-Quality Direct Posterior Composite Restorations - Layering and FinishingPaulina LobosÎncă nu există evaluări
- Posterior Composite Restoration UpdateDocument10 paginiPosterior Composite Restoration UpdateBianca IovoaiaÎncă nu există evaluări
- Some Myths in Dentin Bonding An Evidence Based PerspectiveDocument7 paginiSome Myths in Dentin Bonding An Evidence Based PerspectiveCristian Aguilera100% (1)
- Bopt PanizDocument9 paginiBopt PanizIvan CarreraÎncă nu există evaluări
- Eur JEsthet Dent 2013 MeyenbergDocument97 paginiEur JEsthet Dent 2013 Meyenbergsoma kiranÎncă nu există evaluări
- Pacquet2022 - Therapeutic Strategy For Cracked TeethDocument17 paginiPacquet2022 - Therapeutic Strategy For Cracked TeethJosé Ramón CuetoÎncă nu există evaluări
- Articol L.O.C.Document0 paginiArticol L.O.C.Anda TarasciucÎncă nu există evaluări
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pagini3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilÎncă nu există evaluări
- Optimizing Gingival EstheticsDocument8 paginiOptimizing Gingival EstheticsThe Bioclear Clinic100% (1)
- Implants in Clinical Dentistry PDFDocument274 paginiImplants in Clinical Dentistry PDFCristian AndriescuÎncă nu există evaluări
- Implantology SolutionsDocument22 paginiImplantology SolutionsRAEDÎncă nu există evaluări
- Bonding To Caries Affected DentinDocument13 paginiBonding To Caries Affected DentinJoshua Valdez100% (1)
- Artigo 4Document14 paginiArtigo 4joao pauloÎncă nu există evaluări
- Prepared Cavities On The StrenDocument4 paginiPrepared Cavities On The StrenPriyank RaiÎncă nu există evaluări
- Immediate Dentin Sealing A Literature ReviewDocument24 paginiImmediate Dentin Sealing A Literature ReviewAmin RouhaniÎncă nu există evaluări
- Direct Cuspal CoverageDocument8 paginiDirect Cuspal CoverageLuLu NikhlaturÎncă nu există evaluări
- Drill Less Air AbrasionDocument4 paginiDrill Less Air AbrasionMaria IvanaÎncă nu există evaluări
- 10 1016@j Prosdent 2020 05 007Document5 pagini10 1016@j Prosdent 2020 05 007Anjali DuttaÎncă nu există evaluări
- Blanqueamiento No Vital PDFDocument11 paginiBlanqueamiento No Vital PDFPatricio Alejandro Cornejo Mutizabal100% (1)
- Protocol Clinic Proteze BPS IvoclarDocument38 paginiProtocol Clinic Proteze BPS IvoclarOvidiu SchifirnetÎncă nu există evaluări
- Artículo 2Document10 paginiArtículo 2jhon valdiviezoÎncă nu există evaluări
- The New Science of Strong TeethDocument4 paginiThe New Science of Strong TeethThe Bioclear ClinicÎncă nu există evaluări
- Biologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceDocument21 paginiBiologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceRoopa BabannavarÎncă nu există evaluări
- Silane Adhesion Mechanism in Dental Applications and Surface Treatments - A Review 2018Document16 paginiSilane Adhesion Mechanism in Dental Applications and Surface Treatments - A Review 2018Ariel TocoÎncă nu există evaluări
- Inlay Onlay Parte 222 PDFDocument23 paginiInlay Onlay Parte 222 PDFKhenny Jhynmir Paucar VillegasÎncă nu există evaluări
- Clinical PhotographyDocument6 paginiClinical PhotographyDumitru PopÎncă nu există evaluări
- Deliperi S - PPAD - 2005 PDFDocument9 paginiDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroÎncă nu există evaluări
- Direct Esthetic Restorations Based On Translucency and Opacity of Composite Resins PDFDocument15 paginiDirect Esthetic Restorations Based On Translucency and Opacity of Composite Resins PDFMaricarmen UrbanoÎncă nu există evaluări
- Terry Part-One PDFDocument8 paginiTerry Part-One PDFhptuanamaÎncă nu există evaluări
- Air Abrasion An Emerging Standard of CarDocument25 paginiAir Abrasion An Emerging Standard of CarValeriu IlincaÎncă nu există evaluări
- Multimedia PDFDocument16 paginiMultimedia PDFadamÎncă nu există evaluări
- An Overview of Tooth-BleachingDocument23 paginiAn Overview of Tooth-BleachingRolzilah RohaniÎncă nu există evaluări
- Vandooren Interdisc 2 LeseprobeDocument33 paginiVandooren Interdisc 2 LeseprobeAlfred OrozcoÎncă nu există evaluări
- Ebook: Zirconia: Facts and MisconceptionsDocument9 paginiEbook: Zirconia: Facts and MisconceptionsCaglarBursaÎncă nu există evaluări
- Ceramics As Biomaterials For Dental RestorationDocument17 paginiCeramics As Biomaterials For Dental RestorationCatalina GómezÎncă nu există evaluări
- 1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyDocument4 pagini1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyalbertaugustineÎncă nu există evaluări
- IJEDe 15 03 Rocca 852 2Document22 paginiIJEDe 15 03 Rocca 852 2hannaly estradaÎncă nu există evaluări
- Bioemulation PDFDocument13 paginiBioemulation PDFjotapintor100% (1)
- A Didactic Concept Of: Dental MorphologyDocument9 paginiA Didactic Concept Of: Dental MorphologyErick Brañes Espinoza100% (1)
- INTRAORAL SCANNING Improving Efficiency and Advanced WorkflowDocument15 paginiINTRAORAL SCANNING Improving Efficiency and Advanced WorkflowNguyễn Văn KhươngÎncă nu există evaluări
- Treating The Mother of Black Triangles With Bioclear VeneersDocument4 paginiTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicÎncă nu există evaluări
- Clinical Techniques For Composite PlacementDocument4 paginiClinical Techniques For Composite PlacementRizta RiztiaÎncă nu există evaluări
- Case Report Konser 2Document22 paginiCase Report Konser 2Nisa Ulil AmriÎncă nu există evaluări
- QDT 2001 PDFDocument239 paginiQDT 2001 PDFAlex BurdeÎncă nu există evaluări
- Carvalho Et Al 2021 IJEDDocument19 paginiCarvalho Et Al 2021 IJEDclaudiaÎncă nu există evaluări
- Adhesion of Resin Cement To Dentin Effec PDFDocument12 paginiAdhesion of Resin Cement To Dentin Effec PDFNathaly Granda ZapataÎncă nu există evaluări
- Anterior Veneer Restorations An Evidence-Based Minimal-Intervention PerspectiveDocument20 paginiAnterior Veneer Restorations An Evidence-Based Minimal-Intervention PerspectiveAlex Gutierrez AcostaÎncă nu există evaluări
- Crown Lenghtening - Gummy Smile PDFDocument13 paginiCrown Lenghtening - Gummy Smile PDFVladislava GanevaÎncă nu există evaluări
- (2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKDocument13 pagini(2019) Cervical Margin Relocation - Case Series and New Classification Systems. CHECKBárbara Meza Lewis100% (1)
- Decision-Making Process PDFDocument13 paginiDecision-Making Process PDFVladislava GanevaÎncă nu există evaluări
- Evidence Based Concepts and Procedures For Bonded Inlays and Onlays Part IIIDocument17 paginiEvidence Based Concepts and Procedures For Bonded Inlays and Onlays Part IIIJL' CardosoÎncă nu există evaluări
- WRP Examination Extension 1 2012Document12 paginiWRP Examination Extension 1 2012Belinda JadeÎncă nu există evaluări
- EXP1POSTLABDocument13 paginiEXP1POSTLABGiane MagimotÎncă nu există evaluări
- Food - Forage - Potential - and - Carrying - Capacity - Rusa Kemampo - MedKonDocument9 paginiFood - Forage - Potential - and - Carrying - Capacity - Rusa Kemampo - MedKonRotten AnarchistÎncă nu există evaluări
- Chinese ArchitectureDocument31 paginiChinese Architecturenusantara knowledge100% (2)
- Primakuro Catalogue Preview16-MinDocument10 paginiPrimakuro Catalogue Preview16-MinElizabeth LukitoÎncă nu există evaluări
- Ac 521 007Document10 paginiAc 521 007JacquesÎncă nu există evaluări
- Scuba Diving - Technical Terms MK IDocument107 paginiScuba Diving - Technical Terms MK IJoachim MikkelsenÎncă nu există evaluări
- 1mrk513011-Ben en Auxiliary Current Transformer For Radss 1-Phase and 3-Phase Slce 12 Slce 16 Slxe 4Document4 pagini1mrk513011-Ben en Auxiliary Current Transformer For Radss 1-Phase and 3-Phase Slce 12 Slce 16 Slxe 4GustavoForsterÎncă nu există evaluări
- Ketu in 12th HousesDocument10 paginiKetu in 12th HousesSanket MishraÎncă nu există evaluări
- DIY Paper Sculpture: The PrincipleDocument20 paginiDIY Paper Sculpture: The PrincipleEditorial MosheraÎncă nu există evaluări
- 132kV Substation Feasibility StudyDocument16 pagini132kV Substation Feasibility StudyTafadzwa MurwiraÎncă nu există evaluări
- Catalogue: Packer SystemDocument56 paginiCatalogue: Packer SystemChinmoyee Sharma100% (1)
- The Explanation of The Fundamentals of Islamic BeliefDocument95 paginiThe Explanation of The Fundamentals of Islamic BeliefbooksofthesalafÎncă nu există evaluări
- Refrigeration Engineer Quick ReferenceDocument2 paginiRefrigeration Engineer Quick ReferenceventilationÎncă nu există evaluări
- TC AdvisoryDocument1 paginăTC AdvisoryJerome DelfinoÎncă nu există evaluări
- Primary Three Exam Question.Document17 paginiPrimary Three Exam Question.ogidan preciousÎncă nu există evaluări
- Celly BoostbkDocument15 paginiCelly BoostbknomikabÎncă nu există evaluări
- AnamnezaDocument3 paginiAnamnezaTeodora StevanovicÎncă nu există evaluări
- ONGC Buyout GOI's Entire 51.11% Stake in HPCLDocument4 paginiONGC Buyout GOI's Entire 51.11% Stake in HPCLArpan AroraÎncă nu există evaluări
- Caption Sheet 4-Kailynn BDocument4 paginiCaption Sheet 4-Kailynn Bapi-549116310Încă nu există evaluări
- From Science To God by Peter RussellDocument6 paginiFrom Science To God by Peter RussellFilho adulto pais alcolatrasÎncă nu există evaluări
- Daoyin Physical Calisthenics in The Internal Arts by Sifu Bob Robert Downey Lavericia CopelandDocument100 paginiDaoyin Physical Calisthenics in The Internal Arts by Sifu Bob Robert Downey Lavericia CopelandDragonfly HeilungÎncă nu există evaluări
- Pi 0614 Hiblack f890b en WebDocument2 paginiPi 0614 Hiblack f890b en Web王偉仲Încă nu există evaluări
- Rubber Lined Piping - A Solution To Corrosion ResistanceDocument5 paginiRubber Lined Piping - A Solution To Corrosion ResistanceMohamed AghilaÎncă nu există evaluări
- Leta-Leta CaveDocument5 paginiLeta-Leta CaveToniÎncă nu există evaluări
- 1 Name of Work:-Improvement of Epum Road (Northern Side) Connecting With Imphal-Saikul Road I/c Pucca DrainDocument1 pagină1 Name of Work:-Improvement of Epum Road (Northern Side) Connecting With Imphal-Saikul Road I/c Pucca DrainHemam PrasantaÎncă nu există evaluări
- Web+Presentation+12+July+2016 EA+-+Eric+LumeDocument57 paginiWeb+Presentation+12+July+2016 EA+-+Eric+LumetranthabinÎncă nu există evaluări
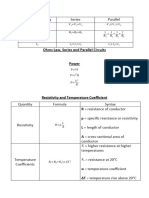
- EET - Formulas - Christmas TermDocument3 paginiEET - Formulas - Christmas TermJMDÎncă nu există evaluări
- Asyb 2020 2Document295 paginiAsyb 2020 2KhangÎncă nu există evaluări
- 2UEB000487 v1 Drive On GeneratorDocument19 pagini2UEB000487 v1 Drive On GeneratorSherifÎncă nu există evaluări