S-ar putea să vă placă și
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersDe la EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersÎncă nu există evaluări
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsDe la EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsÎncă nu există evaluări
- 01-Eyehistory Part2Document3 pagini01-Eyehistory Part2sharu4291Încă nu există evaluări
- Unit Two Basic Examination of The Eye: 2.1. History TakingDocument12 paginiUnit Two Basic Examination of The Eye: 2.1. History TakingiuytrerÎncă nu există evaluări
- Astigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandAstigmatism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- LASIK: A Guide to Laser Vision CorrectionDe la EverandLASIK: A Guide to Laser Vision CorrectionEvaluare: 2.5 din 5 stele2.5/5 (2)
- Nodules: - Chalazion - Acute HordeolaDocument20 paginiNodules: - Chalazion - Acute HordeolaShari' Si WahyuÎncă nu există evaluări
- CH 1 Mental Health Student SlidesDocument29 paginiCH 1 Mental Health Student SlidesHardeep Kaur100% (1)
- Clinical PresentationDocument54 paginiClinical PresentationSêrâphîm HâdíÎncă nu există evaluări
- Anxiety: Clinical Guidelines For The Management ofDocument165 paginiAnxiety: Clinical Guidelines For The Management ofDidina_Ina100% (1)
- Eye Dxtics and Eye DisordersDocument53 paginiEye Dxtics and Eye DisordersJanine Dela CruzÎncă nu există evaluări
- Case PresentationDocument7 paginiCase PresentationDeeksha RawatÎncă nu există evaluări
- Case Studies PresbyopiaDocument33 paginiCase Studies PresbyopiaMalaika ZubairÎncă nu există evaluări
- Dnb-Ophthalmology: Competency Based Training ProgrammeDocument33 paginiDnb-Ophthalmology: Competency Based Training ProgrammeRakhiDcruzÎncă nu există evaluări
- List of Drugs Recommended to М-1 - 2021Document2 paginiList of Drugs Recommended to М-1 - 2021Asma AhmedÎncă nu există evaluări
- Cohen Notes 1Document10 paginiCohen Notes 1api-393109247Încă nu există evaluări
- Psychologi Cal Disorders: Powerpoint ® PresentationDocument86 paginiPsychologi Cal Disorders: Powerpoint ® PresentationZariyah PangilinanÎncă nu există evaluări
- Continue: Stallard's Eye Surgery PDFDocument3 paginiContinue: Stallard's Eye Surgery PDFCod Mobile100% (1)
- Job Description of A Trained and Registered Ophthalmic NurseDocument1 paginăJob Description of A Trained and Registered Ophthalmic NurseKwaku OwusuÎncă nu există evaluări
- Overview of Ophthalmic EquipmentDocument57 paginiOverview of Ophthalmic EquipmenttallrajÎncă nu există evaluări
- Clinical Optometry Primary Eye CareDocument3 paginiClinical Optometry Primary Eye CareDanielle SangalangÎncă nu există evaluări
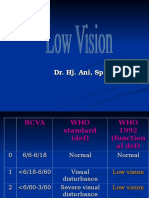
- Low VisionDocument36 paginiLow VisionIqbal HabibieÎncă nu există evaluări
- Chest Tubes: From Indication To RemovalDocument49 paginiChest Tubes: From Indication To Removaldara octavianiÎncă nu există evaluări
- I Co Basic Science ResourcesDocument4 paginiI Co Basic Science ResourcesAlejandra Herrera DíazÎncă nu există evaluări
- Warfarin Dosing PDFDocument3 paginiWarfarin Dosing PDFOMGStudyÎncă nu există evaluări
- Clinical Study On Scleral Lenses by Dr. Elise KramerDocument8 paginiClinical Study On Scleral Lenses by Dr. Elise KramerMiami Contact Lens InstituteÎncă nu există evaluări
- 3280 4.19MB Strabismus - A Decision Making ApproachDocument206 pagini3280 4.19MB Strabismus - A Decision Making ApproachPaulEstrellaÎncă nu există evaluări
- Depression in Older Adults: A Treatable Medical ConditionDocument12 paginiDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- FC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Document2 paginiFC Ophth (SA) Primary IA Past Papers - 2019 1st Semester 18-3-2019Richard100% (1)
- The Pediatric Neurological Exam Chapter by W LoganDocument34 paginiThe Pediatric Neurological Exam Chapter by W LoganStarLink1Încă nu există evaluări
- Visual Field InterpretationDocument52 paginiVisual Field InterpretationUlquiorra Schiffer100% (1)
- Ophthamology Exam NotesDocument132 paginiOphthamology Exam Noteshenry100% (2)
- WSD Brochure Update1Document8 paginiWSD Brochure Update1Fabianto SantosoÎncă nu există evaluări
- NYU PGY-2 Ophthalmology Basics Guide: D1 (3) .GifDocument27 paginiNYU PGY-2 Ophthalmology Basics Guide: D1 (3) .GiftraceyÎncă nu există evaluări
- Refraction and PrescribingDocument6 paginiRefraction and PrescribingawaisÎncă nu există evaluări
- Retinoscopy: Moderator:-Dr. Jyoti PuriDocument33 paginiRetinoscopy: Moderator:-Dr. Jyoti PuriSafa Abdualrahaman Ali HamadÎncă nu există evaluări
- Regulations Relating To The Surgical Fellowship Examination in Ophthalmology Parts 1, 2 and 3Document13 paginiRegulations Relating To The Surgical Fellowship Examination in Ophthalmology Parts 1, 2 and 3NoorÎncă nu există evaluări
- Optometry PresentationDocument11 paginiOptometry PresentationEvelyn Tran100% (1)
- Are The Teachers Responsible For Students FailureDocument1 paginăAre The Teachers Responsible For Students Failuretummalapalli venkateswara rao100% (1)
- Basic Sciences in Ophthalmology - 9788184486087-EmailDocument446 paginiBasic Sciences in Ophthalmology - 9788184486087-EmailwulanfarichahÎncă nu există evaluări
- Opthhalmology Examination ReviewDocument12 paginiOpthhalmology Examination ReviewFaiq Syukri Bin SaparudinÎncă nu există evaluări
- Okap Samson Uveitis PDFDocument12 paginiOkap Samson Uveitis PDFsharu4291Încă nu există evaluări
- Ocular EmergDocument61 paginiOcular EmergKBR RS UNHAS100% (1)
- Cataract Surgery in Retina PatientsDocument21 paginiCataract Surgery in Retina PatientsAnonymous 4OnqyBErÎncă nu există evaluări
- Ocular Anatomy - The RetinaDocument106 paginiOcular Anatomy - The RetinaJaneÎncă nu există evaluări
- Paediatric Handbook - Amanda GweeDocument5 paginiPaediatric Handbook - Amanda GweezekijuraÎncă nu există evaluări
- 014 Duke Elder Examination Information For Candidates 2013Document9 pagini014 Duke Elder Examination Information For Candidates 2013PartialChargeÎncă nu există evaluări
- 19 Rationale of Retinal Detachment ManagementDocument87 pagini19 Rationale of Retinal Detachment ManagementvajasaÎncă nu există evaluări
- Ophthalmic PrismDocument55 paginiOphthalmic PrismHimank RanaÎncă nu există evaluări
- Wound Management Guide DigitalDocument48 paginiWound Management Guide DigitalBrian NiuÎncă nu există evaluări
- How To Read Fluorescein Angiography (Ophthalmology)Document56 paginiHow To Read Fluorescein Angiography (Ophthalmology)yazan100% (9)
- CPG Diabetic RetinopathyDocument49 paginiCPG Diabetic RetinopathyRebecca WongÎncă nu există evaluări
- Foreign Optometrist For CanadaDocument9 paginiForeign Optometrist For CanadaABDUL HAMEEDÎncă nu există evaluări
- Clinical Ophthalmic Oncology Eyelid and Conjunctival TumorsDocument239 paginiClinical Ophthalmic Oncology Eyelid and Conjunctival TumorsRosa SoledadÎncă nu există evaluări
- Scientific Foundations of OphthalmologyDe la EverandScientific Foundations of OphthalmologyEdward S. PerkinsÎncă nu există evaluări
- Viva and Osce Exams in Ophthalmology A Revision Study Guide 1st Ed 9783030430627 9783030430634 CompressDocument392 paginiViva and Osce Exams in Ophthalmology A Revision Study Guide 1st Ed 9783030430627 9783030430634 CompressstingbeesparvÎncă nu există evaluări
- Sdfasdfaadsf Adsf SD F'SDF SD Fs DF SDF S DFSDFDocument1 paginăSdfasdfaadsf Adsf SD F'SDF SD Fs DF SDF S DFSDFaashish_39Încă nu există evaluări
- CodesDocument2 paginiCodesaashish_39Încă nu există evaluări
- Security Issues and Solutions in Cloud ComputingDocument14 paginiSecurity Issues and Solutions in Cloud Computingaashish_39Încă nu există evaluări
- Files-2-Lecture Notes Chapter 3 - System Development MethodologiesDocument26 paginiFiles-2-Lecture Notes Chapter 3 - System Development Methodologiesaashish_39100% (1)
- Security Issues and Solutions in Cloud ComputingDocument14 paginiSecurity Issues and Solutions in Cloud Computingaashish_39Încă nu există evaluări
- 05chap 4 - Research Methodology and DesignDocument44 pagini05chap 4 - Research Methodology and Designaashish_39Încă nu există evaluări
- Cplus 3.0 ManualDocument22 paginiCplus 3.0 Manualaashish_39Încă nu există evaluări
- This Is A Preparatory Course For Seminar in Thesis WritingDocument1 paginăThis Is A Preparatory Course For Seminar in Thesis Writingaashish_39Încă nu există evaluări
- This Is A Preparatory Course For Seminar in Thesis Writing. and This Is Scale 2Document1 paginăThis Is A Preparatory Course For Seminar in Thesis Writing. and This Is Scale 2aashish_39Încă nu există evaluări
- Connecting Through A Cabled Network Communication Media TypesDocument2 paginiConnecting Through A Cabled Network Communication Media Typesaashish_39Încă nu există evaluări
- Moebius Syndrome Due To Prenatal Exposure To MisoprostolDocument4 paginiMoebius Syndrome Due To Prenatal Exposure To Misoprostolaashish_39Încă nu există evaluări
- User Interface Design: Designing Effective Interfaces For Software Systems ObjectivesDocument26 paginiUser Interface Design: Designing Effective Interfaces For Software Systems Objectivesaashish_39Încă nu există evaluări
- This Is A Preparatory Course For Seminar in Thesis Writing. and This Is Scale 2Document1 paginăThis Is A Preparatory Course For Seminar in Thesis Writing. and This Is Scale 2aashish_39Încă nu există evaluări
- Present OneDocument1 paginăPresent Oneaashish_39Încă nu există evaluări
- Preliminaries: What We Will DiscussDocument30 paginiPreliminaries: What We Will Discussaashish_39Încă nu există evaluări
- Smartbro DetailsDocument1 paginăSmartbro Detailsaashish_39Încă nu există evaluări
- Metropolitan Manila Transit Map - Makati City AreaDocument2 paginiMetropolitan Manila Transit Map - Makati City AreanbellosilloÎncă nu există evaluări
- Codes Example NetDocument1 paginăCodes Example Netaashish_39Încă nu există evaluări
- CodesDocument2 paginiCodesaashish_39Încă nu există evaluări
- Adamson University: Tower of Hanoi: Following Are The Steps To Slide Different Size of Disc Onto The Last Rod. Step 1Document2 paginiAdamson University: Tower of Hanoi: Following Are The Steps To Slide Different Size of Disc Onto The Last Rod. Step 1aashish_39Încă nu există evaluări
- Lecture 1 Intro To Programming LanguagesDocument6 paginiLecture 1 Intro To Programming Languagesaashish_39Încă nu există evaluări
- Object Oriented Programming With C#Document65 paginiObject Oriented Programming With C#pramod_y100% (1)
- Moebius Syndrome: by Dr. Bibhuti Thapa First Year Resident, JRRMMCDocument7 paginiMoebius Syndrome: by Dr. Bibhuti Thapa First Year Resident, JRRMMCaashish_39Încă nu există evaluări
- P90X CalendarDocument6 paginiP90X Calendarnejuma91% (34)
- Electrodiagnosis of Retinal Disease: Download Free Full Version EbookDocument1 paginăElectrodiagnosis of Retinal Disease: Download Free Full Version Ebookaashish_39Încă nu există evaluări
- 1 S and 2 S ComplementDocument1 pagină1 S and 2 S ComplementbmshivakumarÎncă nu există evaluări
- Software Engineering TopicsDocument1 paginăSoftware Engineering Topicsaashish_39Încă nu există evaluări
- CheatSheet C# Vs VBdoc PDFDocument16 paginiCheatSheet C# Vs VBdoc PDFRastateÎncă nu există evaluări
- Source Program Source Program: Programming Language - pg.1Document3 paginiSource Program Source Program: Programming Language - pg.1aashish_39Încă nu există evaluări