S-ar putea să vă placă și
- Fix Your Credit Score: Add Up To 100 Points in 30 Days or LessDe la EverandFix Your Credit Score: Add Up To 100 Points in 30 Days or LessÎncă nu există evaluări
- Employment VerificationDocument2 paginiEmployment VerificationthehomemachineÎncă nu există evaluări
- 1040 Exam Prep: Module II - Basic Tax ConceptsDe la Everand1040 Exam Prep: Module II - Basic Tax ConceptsEvaluare: 1.5 din 5 stele1.5/5 (2)
- How to Increase or Build Your Credit Score in One Month: Add Over 100 Points Without The Need of Credit Repair ServicesDe la EverandHow to Increase or Build Your Credit Score in One Month: Add Over 100 Points Without The Need of Credit Repair ServicesEvaluare: 3 din 5 stele3/5 (1)
- EFT Form - FillableDocument3 paginiEFT Form - FillableZachÎncă nu există evaluări
- Enrollment Form FiitjeeDocument16 paginiEnrollment Form FiitjeeGurumurthy KalyanasundaramÎncă nu există evaluări
- Doors & Window Installation - DraftDocument7 paginiDoors & Window Installation - DraftGaneshÎncă nu există evaluări
- Avanse Part Pre Payment Foreclosure Form ELDocument1 paginăAvanse Part Pre Payment Foreclosure Form ELArun KatareÎncă nu există evaluări
- Government Accounting Final Examination With Answer and SolutionDocument13 paginiGovernment Accounting Final Examination With Answer and SolutionRheu Reyes100% (6)
- Promise To PayDocument1 paginăPromise To PayYehezkiel RomartogiÎncă nu există evaluări
- Financial Aid and Loans for Students Crash CourseDe la EverandFinancial Aid and Loans for Students Crash CourseÎncă nu există evaluări
- General Mathematics q2 LasDocument117 paginiGeneral Mathematics q2 LasGian C. GuzmanÎncă nu există evaluări
- Melcs EntrepDocument1 paginăMelcs EntrepErlie100% (5)
- Welcomes You To ISO 19600:2014 Awareness Training ProgrammeDocument119 paginiWelcomes You To ISO 19600:2014 Awareness Training ProgrammeNada HajriÎncă nu există evaluări
- COunter Affidavit EstafaDocument9 paginiCOunter Affidavit EstafaTetet RomeroÎncă nu există evaluări
- Correspondents 23 March 2020Document164 paginiCorrespondents 23 March 2020Nicolas Bernard100% (1)
- Pt. Aldenio Jurnal Penerimaan Kas Bulan: Desember 2016Document52 paginiPt. Aldenio Jurnal Penerimaan Kas Bulan: Desember 2016arum88% (8)
- DU Thirdparty Agreement-Tppa - GenericDocument2 paginiDU Thirdparty Agreement-Tppa - Genericsunoln12Încă nu există evaluări
- 1 Program Withdrawal & Refund Form (Merged)Document2 pagini1 Program Withdrawal & Refund Form (Merged)Hartek BackupÎncă nu există evaluări
- Ta Te TiDocument5 paginiTa Te Tirodel agustinÎncă nu există evaluări
- Adjunct Health Insurance Certification FormDocument2 paginiAdjunct Health Insurance Certification FormElena GerashchenkoÎncă nu există evaluări
- 2013 14 International Student New ContractDocument2 pagini2013 14 International Student New ContracthalovoaÎncă nu există evaluări
- Instructions:: Part 1-Personal InformationDocument7 paginiInstructions:: Part 1-Personal InformationISLAND NATANYAÎncă nu există evaluări
- 2020 Application For Deferral of Tuition Fee PaymentDocument2 pagini2020 Application For Deferral of Tuition Fee PaymentBao Phong TranÎncă nu există evaluări
- Enrollment Agreement SampleDocument4 paginiEnrollment Agreement SamplemasroorimsÎncă nu există evaluări
- Refund Form NS41960Document3 paginiRefund Form NS41960Rajveer KaurÎncă nu există evaluări
- AMS Client Services Agreement VFDocument5 paginiAMS Client Services Agreement VFGary AndersonÎncă nu există evaluări
- University of Central Florida Student Health Insurance PlanDocument1 paginăUniversity of Central Florida Student Health Insurance PlanHussain AbouelkhairÎncă nu există evaluări
- Paychex Direct Deposit Authorization FormDocument1 paginăPaychex Direct Deposit Authorization FormThierry NhamoÎncă nu există evaluări
- USCredit ApplicationDocument5 paginiUSCredit ApplicationFSO COMPRESORESÎncă nu există evaluări
- Personal Bond Refund Application FormDocument2 paginiPersonal Bond Refund Application FormNUR SUHANA HAMZAHÎncă nu există evaluări
- DATE: To: FROM: April 6, 2009 Director of A LicensedDocument29 paginiDATE: To: FROM: April 6, 2009 Director of A Licensedapi-26136370Încă nu există evaluări
- Automatic Payment Authorization FormDocument1 paginăAutomatic Payment Authorization Formkaiser55Încă nu există evaluări
- Authorization For Direct PaymentDocument1 paginăAuthorization For Direct Paymentheidilynpanter7121Încă nu există evaluări
- Volunteer Form SampleDocument2 paginiVolunteer Form SampleJeffrey BlissiÎncă nu există evaluări
- Election Form and Compensation Reduction Agreement: Sagitec Solutions LLCDocument2 paginiElection Form and Compensation Reduction Agreement: Sagitec Solutions LLCFinding FannyÎncă nu există evaluări
- Fall 20 - Spring 20 - Summer 20 - : Select TermDocument2 paginiFall 20 - Spring 20 - Summer 20 - : Select TermAnjuChackungalÎncă nu există evaluări
- Fall2011Payment Plan ApplicationDocument3 paginiFall2011Payment Plan ApplicationAkinbode Sunday OluwagbengaÎncă nu există evaluări
- Description: Tags: DLB0341AttDocument1 paginăDescription: Tags: DLB0341Attanon-404473Încă nu există evaluări
- Bank Debit Order Instruction Form/Credit Request: MandateDocument1 paginăBank Debit Order Instruction Form/Credit Request: MandateAtulÎncă nu există evaluări
- Description: Tags: DLB0341AttDocument1 paginăDescription: Tags: DLB0341Attanon-952530Încă nu există evaluări
- ML 1Document1 paginăML 1Angelique Marie Adriano100% (1)
- WT Form 19Document2 paginiWT Form 19sukanyaÎncă nu există evaluări
- Rental App - PrimaryDocument3 paginiRental App - Primaryapi-335836813Încă nu există evaluări
- College Payment Agreement-WPS OfficeDocument3 paginiCollege Payment Agreement-WPS OfficePedro Pablo Mederos FragaÎncă nu există evaluări
- StoneX Employee Direct Deposit FormDocument2 paginiStoneX Employee Direct Deposit Formz44pzw2hmxÎncă nu există evaluări
- Certificate of Non-EnrollmentDocument1 paginăCertificate of Non-EnrollmentIan PalmaÎncă nu există evaluări
- Extension in Payment of FeeDocument3 paginiExtension in Payment of FeeAmrit Pal SinghÎncă nu există evaluări
- Truist Ach FormDocument1 paginăTruist Ach FormhugstinsÎncă nu există evaluări
- MAHSA University Global Mobility FormDocument4 paginiMAHSA University Global Mobility FormEdgar ZetaÎncă nu există evaluări
- Revised 2020 - SLP Application FormDocument2 paginiRevised 2020 - SLP Application FormMaffi Gieson AsilumÎncă nu există evaluări
- Income Withholding For SupportDocument3 paginiIncome Withholding For SupportballÎncă nu există evaluări
- 2022 Grade 456 7 School Fee Commitment FormDocument5 pagini2022 Grade 456 7 School Fee Commitment FormJanice MkhizeÎncă nu există evaluări
- Ag 501Document2 paginiAg 501Cindy FazzinoÎncă nu există evaluări
- Membership ApplicationDocument1 paginăMembership Applicationashley1259Încă nu există evaluări
- Es2606 Adobe11Document1 paginăEs2606 Adobe11marsha granthamÎncă nu există evaluări
- Alorica at Home Wage Payment Election and Consent FormDocument2 paginiAlorica at Home Wage Payment Election and Consent Formydnahr zuegirdorÎncă nu există evaluări
- Financial InformationDocument1 paginăFinancial InformationMykayla KerrÎncă nu există evaluări
- Cancellation FormDocument2 paginiCancellation FormAkash TebaliyaÎncă nu există evaluări
- Dependent Care: How To File A Claim For ApprovalDocument2 paginiDependent Care: How To File A Claim For ApprovallogradloÎncă nu există evaluări
- Refund Request Form - Vocational (05-20)Document3 paginiRefund Request Form - Vocational (05-20)deborichiÎncă nu există evaluări
- 2011-12 Campus Employment Application: WWW - Carrollu.edu/prospective/finaid - Employment - AspDocument2 pagini2011-12 Campus Employment Application: WWW - Carrollu.edu/prospective/finaid - Employment - AspJenni VuÎncă nu există evaluări
- Calamity HMDFDocument3 paginiCalamity HMDFchennieÎncă nu există evaluări
- Cps Deferment FormDocument1 paginăCps Deferment Form1tonsilsÎncă nu există evaluări
- Monthly Parking AgreementDocument1 paginăMonthly Parking AgreementClara agathaÎncă nu există evaluări
- Fall 2021 Campus Tour - Saturday 21st AugDocument10 paginiFall 2021 Campus Tour - Saturday 21st AugTimmy OngÎncă nu există evaluări
- Novel of Life 1 - Act 1Document6 paginiNovel of Life 1 - Act 1Timmy OngÎncă nu există evaluări
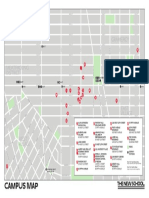
- TNS Campus Map 2021Document1 paginăTNS Campus Map 2021Timmy OngÎncă nu există evaluări
- Better This Way - Production DocumentsDocument15 paginiBetter This Way - Production DocumentsTimmy OngÎncă nu există evaluări
- Speech Lab Texts and NotesDocument2 paginiSpeech Lab Texts and NotesTimmy OngÎncă nu există evaluări
- Novel of Life 2Document12 paginiNovel of Life 2Timmy OngÎncă nu există evaluări
- Questions For ColinDocument2 paginiQuestions For ColinTimmy OngÎncă nu există evaluări
- Timmy Ong - Monologue Acting NotesDocument2 paginiTimmy Ong - Monologue Acting NotesTimmy OngÎncă nu există evaluări
- Global Drama 2 - List of Reading MaterialsDocument2 paginiGlobal Drama 2 - List of Reading MaterialsTimmy OngÎncă nu există evaluări
- Co LabDocument1 paginăCo LabTimmy OngÎncă nu există evaluări
- Outer Ring of Given Circumstances - SalomeDocument5 paginiOuter Ring of Given Circumstances - SalomeTimmy OngÎncă nu există evaluări
- Playground Gang QuestionnaireDocument2 paginiPlayground Gang QuestionnaireTimmy OngÎncă nu există evaluări
- Three Word Sentence StoryDocument2 paginiThree Word Sentence StoryTimmy OngÎncă nu există evaluări
- The Alexander Technique QuestionnaireDocument3 paginiThe Alexander Technique QuestionnaireTimmy OngÎncă nu există evaluări
- Ibsen Research For Scene StudyDocument1 paginăIbsen Research For Scene StudyTimmy OngÎncă nu există evaluări
- Week 3 - ChristDocument2 paginiWeek 3 - ChristTimmy OngÎncă nu există evaluări
- Hamletmachine HomeworkDocument4 paginiHamletmachine HomeworkTimmy OngÎncă nu există evaluări
- Ode To The Shan-Shan - Alexis FedorDocument1 paginăOde To The Shan-Shan - Alexis FedorTimmy OngÎncă nu există evaluări
- Vocal Wisdom: Giovanni Battista LampertiDocument6 paginiVocal Wisdom: Giovanni Battista LampertiTimmy OngÎncă nu există evaluări
- Group Work - Intro (Global Performance in Context)Document7 paginiGroup Work - Intro (Global Performance in Context)Timmy OngÎncă nu există evaluări
- Int. Jerome'S Bedroom - Morning 1 1Document6 paginiInt. Jerome'S Bedroom - Morning 1 1Timmy OngÎncă nu există evaluări
- Week 2 - The Black DoctorDocument1 paginăWeek 2 - The Black DoctorTimmy OngÎncă nu există evaluări
- Week 2 - BrechtDocument1 paginăWeek 2 - BrechtTimmy OngÎncă nu există evaluări
- 2020 2021 University Academic Calendar 1 19 PDFDocument1 pagină2020 2021 University Academic Calendar 1 19 PDFErin May CochancoÎncă nu există evaluări
- Henrik Ibsen and - His ContemporariesDocument12 paginiHenrik Ibsen and - His ContemporariesTimmy OngÎncă nu există evaluări
- The KeyDocument4 paginiThe KeyTimmy OngÎncă nu există evaluări
- 2020-2021 University Academic Calendar Nov19Document1 pagină2020-2021 University Academic Calendar Nov19Timmy OngÎncă nu există evaluări
- Fall 2020 FaqDocument3 paginiFall 2020 FaqTimmy OngÎncă nu există evaluări
- Ibsen Research For Scene StudyDocument1 paginăIbsen Research For Scene StudyTimmy OngÎncă nu există evaluări
- Questions For ColinDocument2 paginiQuestions For ColinTimmy OngÎncă nu există evaluări
- Sherzod SSRN IndustrialPolicyandWTObookDocument37 paginiSherzod SSRN IndustrialPolicyandWTObookSigna PrakuswaÎncă nu există evaluări
- SHRM ReviewDocument18 paginiSHRM ReviewjirnalÎncă nu există evaluări
- 2000 2001 PDFDocument1.272 pagini2000 2001 PDFmuhammad aliÎncă nu există evaluări
- OB Chapter 1Document44 paginiOB Chapter 1habteÎncă nu există evaluări
- Softlogic Finance Brief MemoDocument5 paginiSoftlogic Finance Brief Memomonomono90Încă nu există evaluări
- A Debt-Fuelled Spree That Led To $5.4B PharmEasy's Catch-22 - The KenDocument1 paginăA Debt-Fuelled Spree That Led To $5.4B PharmEasy's Catch-22 - The KenKrish PatelÎncă nu există evaluări
- Agoda Seawind Resort BookingDocument2 paginiAgoda Seawind Resort BookingJayjay FarconÎncă nu există evaluări
- Research Methodology: Dr. Eisha KhanDocument12 paginiResearch Methodology: Dr. Eisha KhanTushar KambojÎncă nu există evaluări
- Business FinanceDocument221 paginiBusiness FinanceMatthew GonzalesÎncă nu există evaluări
- Cost Systems and Cost AccumulationDocument25 paginiCost Systems and Cost AccumulationPrima Warta SanthaliaÎncă nu există evaluări
- RESUME UPD - 1670820102755 - Chinmay Vithal ChavanDocument3 paginiRESUME UPD - 1670820102755 - Chinmay Vithal ChavanRahul PatankarÎncă nu există evaluări
- Australian Sharemarket: TablesDocument20 paginiAustralian Sharemarket: TablesallegreÎncă nu există evaluări
- Plastic Waste Awareness PDFDocument23 paginiPlastic Waste Awareness PDFLasya ThakurÎncă nu există evaluări
- Cortar GST CertificateDocument3 paginiCortar GST CertificatevirajÎncă nu există evaluări
- Xerox-Od Xerox-Od1 MergedDocument2 paginiXerox-Od Xerox-Od1 MergedFor My YouTubeÎncă nu există evaluări
- IJRPR6250Document3 paginiIJRPR6250dienanurbasyithahÎncă nu există evaluări
- A'lla Zahwa Andewi Nugraheni - 464977 - Tugas FM CH 14 & 15Document7 paginiA'lla Zahwa Andewi Nugraheni - 464977 - Tugas FM CH 14 & 15PRA MBAÎncă nu există evaluări
- D NUli RONz 7 G DZ02 Ju Txum PAWu VMQZZ VNXW RxnuceDocument83 paginiD NUli RONz 7 G DZ02 Ju Txum PAWu VMQZZ VNXW RxnucemibeÎncă nu există evaluări
- Product Life Cycle Theory Its Connection With FDIDocument2 paginiProduct Life Cycle Theory Its Connection With FDImohdadib0960% (10)
- AV-OP-06 Manufacturing Iss 1Document4 paginiAV-OP-06 Manufacturing Iss 1Kevin DeLimaÎncă nu există evaluări
- A1 - Sample - 2020 - Strategic Management - Aviation and TourismDocument16 paginiA1 - Sample - 2020 - Strategic Management - Aviation and TourismElroy RodriguesÎncă nu există evaluări
- Tutorial 2 Topic 2: Residence Status of IndividualsDocument3 paginiTutorial 2 Topic 2: Residence Status of Individualsfujinlim98Încă nu există evaluări