S-ar putea să vă placă și
- Melanotropic Peptides: What Exactly Is Meant by "Melanotan"?Document2 paginiMelanotropic Peptides: What Exactly Is Meant by "Melanotan"?Melvin OnyiaÎncă nu există evaluări
- Mechanism of Hormone ActionDocument30 paginiMechanism of Hormone ActionWhite SnelliÎncă nu există evaluări
- ReceptorsDocument9 paginiReceptorsrajenderÎncă nu există evaluări
- Self Harm in AdolescenceDocument2 paginiSelf Harm in AdolescenceAmanda BrunerÎncă nu există evaluări
- AP Bio Ch. 11 Cell CommunicationDocument78 paginiAP Bio Ch. 11 Cell CommunicationRavider JadejaÎncă nu există evaluări
- Fluid Infusion Rates For Pediatric Diabetic Ketoacidosis: David R. Freyer, D.ODocument4 paginiFluid Infusion Rates For Pediatric Diabetic Ketoacidosis: David R. Freyer, D.OFiya Putri ZadaÎncă nu există evaluări
- Heterogeneity of T1DM Raises Questions For Therapy: Paolo PozzilliDocument3 paginiHeterogeneity of T1DM Raises Questions For Therapy: Paolo PozzilliHovhannes SahakyanÎncă nu există evaluări
- Levels of Fecal Calprotectin and The Severity of Postoperative Patients With Crohn's DiseaseDocument2 paginiLevels of Fecal Calprotectin and The Severity of Postoperative Patients With Crohn's DiseaseNejc KovačÎncă nu există evaluări
- EditorialDocument2 paginiEditorialsebastoto778Încă nu există evaluări
- Nej MC 1513316Document4 paginiNej MC 1513316anggiÎncă nu există evaluări
- Catatan MataDocument2 paginiCatatan MataFausiah Ulva MÎncă nu există evaluări
- 5 Cole 07 Jama 297 2351Document9 pagini5 Cole 07 Jama 297 2351CoralineÎncă nu există evaluări
- Genetic Association Study of Putative Functional Single Nucleotide Polymorphisms of Genes in Folate Metabolism and Spina BifidaDocument11 paginiGenetic Association Study of Putative Functional Single Nucleotide Polymorphisms of Genes in Folate Metabolism and Spina BifidaMauro Porcel de PeraltaÎncă nu există evaluări
- 1 s2.0 S0145212612004456 MainDocument9 pagini1 s2.0 S0145212612004456 MainMilana PerkovićÎncă nu există evaluări
- On Theophylline, Leukocytes, and Chicken SoupDocument2 paginiOn Theophylline, Leukocytes, and Chicken SouphdhdhdhdÎncă nu există evaluări
- Zhuo 2012Document7 paginiZhuo 2012mandanatrisaviÎncă nu există evaluări
- Editorial: DNA Damage: Health and LongevityDocument2 paginiEditorial: DNA Damage: Health and LongevityAngelica CobosÎncă nu există evaluări
- Nihms 1523522Document29 paginiNihms 1523522Irvin MarcelÎncă nu există evaluări
- Dna Methylation in Human Diseases: SciencedirectDocument8 paginiDna Methylation in Human Diseases: SciencedirectKarim KACEMÎncă nu există evaluări
- Memantine Updating A Rare Success StoryDocument23 paginiMemantine Updating A Rare Success Storynoucici0Încă nu există evaluări
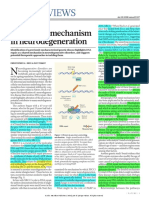
- News & Views: A Unifying Mechanism in NeurodegenerationDocument2 paginiNews & Views: A Unifying Mechanism in Neurodegenerationrocambolescas perthÎncă nu există evaluări
- Nihms 1874250Document35 paginiNihms 1874250foodiejulian1994Încă nu există evaluări
- Journal Pbio 3000850Document33 paginiJournal Pbio 3000850Juan David Pardo Mr. PostmanÎncă nu există evaluări
- The DNA Damage Response Pathways - at The Crossroad of Protein ModificationsDocument9 paginiThe DNA Damage Response Pathways - at The Crossroad of Protein Modificationsshaheena ahmedÎncă nu există evaluări
- Photodynamic Therapy For The Palliation of EsophagDocument2 paginiPhotodynamic Therapy For The Palliation of EsophaglaperaÎncă nu există evaluări
- Brazilian Wasp Venom Kills Cancer Cells by Opening Them UpDocument10 paginiBrazilian Wasp Venom Kills Cancer Cells by Opening Them UpAlf. Andres I. KarrnakisÎncă nu există evaluări
- Sharp 1998Document12 paginiSharp 1998jackashcaÎncă nu există evaluări
- Lee Et Al-2009-Experimental & Molecular MedicineDocument6 paginiLee Et Al-2009-Experimental & Molecular MedicineMauro Porcel de PeraltaÎncă nu există evaluări
- Cancer 07Document9 paginiCancer 07Sayantan DattaÎncă nu există evaluări
- Pi Is 0085253815559528Document4 paginiPi Is 0085253815559528Surya HadiÎncă nu există evaluări
- Introduction To Gene Therapy: 1.1 Genes As DrugsDocument7 paginiIntroduction To Gene Therapy: 1.1 Genes As DrugsJason LingÎncă nu există evaluări
- Clinical Genetics - 2011 - Kanwal - Epigenetic Modifications in CancerDocument9 paginiClinical Genetics - 2011 - Kanwal - Epigenetic Modifications in Cancerpharm.ajbashirÎncă nu există evaluări
- (14796813 - Journal of Molecular Endocrinology) The Retinol Acid Receptor B Gene Is Hypermethylated in Patients With Familial Partial LipodystrophyDocument9 pagini(14796813 - Journal of Molecular Endocrinology) The Retinol Acid Receptor B Gene Is Hypermethylated in Patients With Familial Partial LipodystrophyJovicaÎncă nu există evaluări
- Hydrogen: Another Gas With Therapeutic Potential: James F. George and Anupam AgarwalDocument3 paginiHydrogen: Another Gas With Therapeutic Potential: James F. George and Anupam AgarwalannisaarrumÎncă nu există evaluări
- J1. Effect of Glycated Albumin and Cranberry Components On Interleukin-6 and Matrix Metalloproteinase-3 Production by Human Gingival FibroblastsDocument9 paginiJ1. Effect of Glycated Albumin and Cranberry Components On Interleukin-6 and Matrix Metalloproteinase-3 Production by Human Gingival FibroblastsDwi Dayanti AgustinaÎncă nu există evaluări
- Cancer Science - 2022 - Wang - The Emerging Multifaceted Role of PINK1 in Cancer BiologyDocument11 paginiCancer Science - 2022 - Wang - The Emerging Multifaceted Role of PINK1 in Cancer BiologyT Smith AndresÎncă nu există evaluări
- 3607-Article Text-13375-1-10-20200722Document3 pagini3607-Article Text-13375-1-10-20200722sario indriayaniÎncă nu există evaluări
- TKF 2Document4 paginiTKF 2api-257045584Încă nu există evaluări
- Diagnostic Molecular BiologyDocument2 paginiDiagnostic Molecular Biologythị sô phiaÎncă nu există evaluări
- Functional Activity of Neutrophils and Systemic Inflammatory Response of Down's Syndrome Patients With Periodontal DiseaseDocument6 paginiFunctional Activity of Neutrophils and Systemic Inflammatory Response of Down's Syndrome Patients With Periodontal DiseasegugicevdzoceÎncă nu există evaluări
- OncogenesDocument2 paginiOncogenesSuxy TjoÎncă nu există evaluări
- DNA Repair in Cancer InitiationDocument6 paginiDNA Repair in Cancer InitiationYuanita AndrianiÎncă nu există evaluări
- Microglial Inflammation and Phagocytosis in Alzheimer's Disease: Potential Therapeutic TargetsDocument18 paginiMicroglial Inflammation and Phagocytosis in Alzheimer's Disease: Potential Therapeutic TargetsChristina MountakiÎncă nu există evaluări
- Free Drug Samples and The Opioid CrisisDocument2 paginiFree Drug Samples and The Opioid CrisisNazly ÁlvarezÎncă nu există evaluări
- British Journal Hematology AML TrialDocument10 paginiBritish Journal Hematology AML TrialRahul B SÎncă nu există evaluări
- Therapy Induced Mutagenesis in Relapsed ALL Is Supported by Mutatio - 2020 - BloDocument3 paginiTherapy Induced Mutagenesis in Relapsed ALL Is Supported by Mutatio - 2020 - BloJose Luis Agudelo MosqueraÎncă nu există evaluări
- Mtap Hematology Assesment Quiz 1Document26 paginiMtap Hematology Assesment Quiz 1Jairo Wayne TablacÎncă nu există evaluări
- Genetics and Calcium Nephrolithiasis: Kidney International October 2010Document8 paginiGenetics and Calcium Nephrolithiasis: Kidney International October 2010Marisa IzzaÎncă nu există evaluări
- CNCR 21619Document7 paginiCNCR 21619Syed Shah MuhammadÎncă nu există evaluări
- Duchenne Muscular Dystrophy or Meryon's Disease - LaDocument1 paginăDuchenne Muscular Dystrophy or Meryon's Disease - LaGustavo Dullius MentzÎncă nu există evaluări
- Review: Epigenetics in Human Obesity and Type 2 DiabetesDocument17 paginiReview: Epigenetics in Human Obesity and Type 2 DiabetesStephany BoninÎncă nu există evaluări
- JA A D: Saabg@health - Missouri.eduDocument3 paginiJA A D: Saabg@health - Missouri.eduValentina AdindaÎncă nu există evaluări
- Articulo 4Document2 paginiArticulo 4Evelyn Jiménez MacharéÎncă nu există evaluări
- Ragvin PNAS10Document6 paginiRagvin PNAS10Fernando CasaresÎncă nu există evaluări
- Mutagenesis 2002 Collins 489 93Document5 paginiMutagenesis 2002 Collins 489 93strayassÎncă nu există evaluări
- Alzheimer's Disease: Mark N. Levine, M.DDocument2 paginiAlzheimer's Disease: Mark N. Levine, M.Dlala_bojaÎncă nu există evaluări
- Steroid For AINDocument3 paginiSteroid For AINGadisa DejeneÎncă nu există evaluări
- Paediatrica Indonesiana: Mikhael Yosia, Pustika Amalia WahidiyatDocument8 paginiPaediatrica Indonesiana: Mikhael Yosia, Pustika Amalia WahidiyatNoor Rizka YuliaÎncă nu există evaluări
- Epigenetics As A Modifiable Risk Factor in Periodontal DiseaseDocument15 paginiEpigenetics As A Modifiable Risk Factor in Periodontal DiseaseInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Differentiation: Jennifer E. Bestman, Krista D. Stackley, Jennifer J. Rahn, Tucker J. Williamson, Sherine S. L. ChanDocument19 paginiDifferentiation: Jennifer E. Bestman, Krista D. Stackley, Jennifer J. Rahn, Tucker J. Williamson, Sherine S. L. ChanZeninJosepVásquezVillarÎncă nu există evaluări
- 1 s2.0 S2531137920313067 MainDocument4 pagini1 s2.0 S2531137920313067 MainDinda NajwaÎncă nu există evaluări
- NIH Public Access: Adipose Tissue Attracts and Protects Acute Lymphoblastic Leukemia Cells From ChemotherapyDocument15 paginiNIH Public Access: Adipose Tissue Attracts and Protects Acute Lymphoblastic Leukemia Cells From ChemotherapyFERNANDAÎncă nu există evaluări
- The EMBO Journal - 2022 - Han - Gut Colonization by Bacteroides Requires Translation by An EF G Paralog Lacking GTPaseDocument20 paginiThe EMBO Journal - 2022 - Han - Gut Colonization by Bacteroides Requires Translation by An EF G Paralog Lacking GTPasesethÎncă nu există evaluări
- (Methods in Enzymology 529) Jon Lorsch (Eds.) - Laboratory Methods in Enzymology - DNA-Academic Press (2013)Document379 pagini(Methods in Enzymology 529) Jon Lorsch (Eds.) - Laboratory Methods in Enzymology - DNA-Academic Press (2013)Gabriela QueirozÎncă nu există evaluări
- Kawazu Et Al 2012 - Transforming Mutations of Rac GTP in Human CancersDocument6 paginiKawazu Et Al 2012 - Transforming Mutations of Rac GTP in Human CancersHernestoÎncă nu există evaluări
- Proteins and Cell Regulation Vol 03 - RHO Family GTPases, 1E (2005)Document306 paginiProteins and Cell Regulation Vol 03 - RHO Family GTPases, 1E (2005)DiahaÎncă nu există evaluări
- The Cell Biology of Parkinson's Disease 2021Document31 paginiThe Cell Biology of Parkinson's Disease 2021Carlos Henrique JardimÎncă nu există evaluări
- Chapter 15 SummaryDocument27 paginiChapter 15 SummaryCharlotteÎncă nu există evaluări
- Antiviral Research: François Ferron, Etienne Decroly, Barbara Selisko, Bruno CanardDocument11 paginiAntiviral Research: François Ferron, Etienne Decroly, Barbara Selisko, Bruno CanardJose QuinteroÎncă nu există evaluări
- Davis Et Al - 2013 - Rac1 P29S Is A Spontaneously Activating Cancer Associated GTPase - COS7 CellsDocument6 paginiDavis Et Al - 2013 - Rac1 P29S Is A Spontaneously Activating Cancer Associated GTPase - COS7 CellsHernestoÎncă nu există evaluări
- 2abc PDFDocument62 pagini2abc PDFsriwidiaÎncă nu există evaluări
- Rho GTPases in Cell BiologyDocument8 paginiRho GTPases in Cell BiologyAndrés Alejandro Palma ValenciaÎncă nu există evaluări
- Computational Cell Biology Second ThemeDocument5 paginiComputational Cell Biology Second ThemeGifty RenacidoÎncă nu există evaluări
- G-protein-Coupled ReceptorsDocument24 paginiG-protein-Coupled ReceptorsNaimi Amalia hatimahÎncă nu există evaluări
- Rho-Family Gtpases: It'S Not Only Rac and Rho (And I Like It)Document12 paginiRho-Family Gtpases: It'S Not Only Rac and Rho (And I Like It)Akhilesh SinghÎncă nu există evaluări
- Acetylcholine and Cholinergic Receptors: David A. BrownDocument10 paginiAcetylcholine and Cholinergic Receptors: David A. BrownfahmiÎncă nu există evaluări
- The Role of The Cytoskeletal Protein, Tubulin, in The Mode of Action and Mechanism of Drug Resistance To BenzimidazolesDocument52 paginiThe Role of The Cytoskeletal Protein, Tubulin, in The Mode of Action and Mechanism of Drug Resistance To BenzimidazolesNguyễn Quang LInhÎncă nu există evaluări
- Tyrosine Kinase Receptors in Oncology: Molecular SciencesDocument48 paginiTyrosine Kinase Receptors in Oncology: Molecular SciencesAnuradha Monga KapoorÎncă nu există evaluări
- Enzyme Linked Receptors LectureDocument52 paginiEnzyme Linked Receptors LectureJason PastisÎncă nu există evaluări
- Control of Migration in Tissue EngineeringDocument29 paginiControl of Migration in Tissue EngineeringHarini BalasubramanianÎncă nu există evaluări
- Signal Transduction in Prokaryotes and Eukaryotes-FinalDocument66 paginiSignal Transduction in Prokaryotes and Eukaryotes-FinalAsif gill0% (1)
- Targeting The Untargetable KRAS in Cancer Therapy: Acta Pharmaceutica Sinica BDocument9 paginiTargeting The Untargetable KRAS in Cancer Therapy: Acta Pharmaceutica Sinica Bmothi lalÎncă nu există evaluări
- The Role of Isoforms of Soluble Guanylyl Cyclase in Relaxation of Vascular Smooth Muscle Cells and Corpora Cavernosa - ThesisKellyDecaluweDocument246 paginiThe Role of Isoforms of Soluble Guanylyl Cyclase in Relaxation of Vascular Smooth Muscle Cells and Corpora Cavernosa - ThesisKellyDecaluweCarlos LabradaÎncă nu există evaluări
- 1 2 Receptor Tyrosine Kinases 2021Document44 pagini1 2 Receptor Tyrosine Kinases 2021Bilakovics NoemiÎncă nu există evaluări
- Pengaruh Hiperglemi Terhadap Peran Sitoskeleton (Cytoskeleton) Sebagai Jalur Transduksi Signal (Signal Transduction)Document15 paginiPengaruh Hiperglemi Terhadap Peran Sitoskeleton (Cytoskeleton) Sebagai Jalur Transduksi Signal (Signal Transduction)Syarif HidayatÎncă nu există evaluări
- The Identification of OncogenesDocument43 paginiThe Identification of OncogenesRicha PandeyÎncă nu există evaluări
- Unacademy 4 PDFDocument16 paginiUnacademy 4 PDFANUPAM ANAND KUMAR PANDEY MBA-IÎncă nu există evaluări
- Signal Transduction & G Protein-Coupled Receptors: TopicsDocument33 paginiSignal Transduction & G Protein-Coupled Receptors: TopicsEria MarinaÎncă nu există evaluări
- 23 1099 1 PB PDFDocument11 pagini23 1099 1 PB PDFmuhammad arjoniÎncă nu există evaluări