S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Chemistry in Our Life - Chemicals in MedicinesDocument9 paginiChemistry in Our Life - Chemicals in MedicinesNafis AhmadÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Lunar Drug Study Optha Last RotationDocument4 paginiLunar Drug Study Optha Last RotationGlizzel Jade GumadeÎncă nu există evaluări
- LevofloxacinDocument2 paginiLevofloxacinEliza Rahardja100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Guoying Wang, Guo ZhaoDocument17 paginiGuoying Wang, Guo ZhaoHQ HQÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Tabel Zona Sensitivitas Antibiotik: 1. Enterobactericeae (Klebsiella SP., E.coli, Proteus SP.,)Document7 paginiTabel Zona Sensitivitas Antibiotik: 1. Enterobactericeae (Klebsiella SP., E.coli, Proteus SP.,)puriartini-1Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Long Quiz Antimicrobials Antifungals Antituberculosis AnticancerDocument5 paginiLong Quiz Antimicrobials Antifungals Antituberculosis AnticancerJen PanganibanÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Newer Antibiotics: Guide: DR Saroja A ODocument51 paginiNewer Antibiotics: Guide: DR Saroja A OparahulÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Org MedicinalsDocument24 paginiOrg MedicinalslemtechÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- 5) General BacteriologyDocument86 pagini5) General BacteriologyIanBiagtanÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Acute Simple Cystitis in Women - UpToDateDocument29 paginiAcute Simple Cystitis in Women - UpToDateMédico NautaÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Artikel Ilmiah Priyanto 1Document7 paginiArtikel Ilmiah Priyanto 1yudhit bessieÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- 4 - PnevmoniiDocument49 pagini4 - PnevmoniiPetreÎncă nu există evaluări
- Khameneh 2019Document28 paginiKhameneh 2019Monyet...Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Mechanism of AB ResistanceDocument31 paginiMechanism of AB ResistancesarasatiwanamiÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- FARAD Digest: Egg Residue Considerations During The Treatment of Backyard PoultryDocument8 paginiFARAD Digest: Egg Residue Considerations During The Treatment of Backyard Poultryjust joseÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Age 76 Years Old: 1. Tobacco 2. Alcohol 3. OTC-drugs/ Non-Prescription DrugsDocument42 paginiAge 76 Years Old: 1. Tobacco 2. Alcohol 3. OTC-drugs/ Non-Prescription DrugsJamal Tango Alawiya100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Jase Medical Antibiotic GuideDocument33 paginiJase Medical Antibiotic GuideelectronicoscaldasÎncă nu există evaluări
- Product Knowledge (2) (26-8) 2-1Document38 paginiProduct Knowledge (2) (26-8) 2-1zeyad1234ali0Încă nu există evaluări
- Synthetic Antibacterial AgentsDocument58 paginiSynthetic Antibacterial AgentsApurba Sarker Apu100% (3)
- Treatment of Chlamydia Trachomatis InfectionDocument23 paginiTreatment of Chlamydia Trachomatis InfectionAmbarÎncă nu există evaluări
- Microbiology AssignmentDocument18 paginiMicrobiology AssignmentADITYAROOP PATHAKÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Antiseptics and DisinfectantsDocument79 paginiAntiseptics and Disinfectantssri ram100% (1)
- AntibioticsDocument122 paginiAntibioticsdentistry24100% (1)
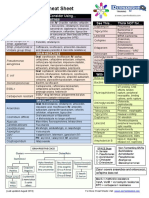
- Antibiotic Study Cheat Sheet August 2019Document1 paginăAntibiotic Study Cheat Sheet August 2019Ryan TurnerÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Translate 5Document22 paginiTranslate 5Dahliawati MohiÎncă nu există evaluări
- Levofloxacin 500mg Film-Coated Tablets - Summary of Product Characteristics (SMPC)Document10 paginiLevofloxacin 500mg Film-Coated Tablets - Summary of Product Characteristics (SMPC)OdunlamiÎncă nu există evaluări
- QuinolonesDocument24 paginiQuinolonesKevin ArechigaÎncă nu există evaluări
- DR - Kima PresentationDocument49 paginiDR - Kima Presentationdvo aizawlÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Fluoroquinolone Drug StudyDocument3 paginiFluoroquinolone Drug StudyEmagra AzilÎncă nu există evaluări
- INDEXDocument16 paginiINDEXayush rajeshÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)