S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- TSH TestDocument5 paginiTSH TestdenalynÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Suicide Prevention BrochureDocument2 paginiSuicide Prevention Brochureapi-288157545Încă nu există evaluări
- Cassandra Training 3 Day CourseDocument5 paginiCassandra Training 3 Day CoursedsunteÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Cns Spectrums: The Clinical Challenges of Akathisia CME Review ArticleDocument16 paginiCns Spectrums: The Clinical Challenges of Akathisia CME Review Articledzakiyah nurul israÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- m100 Resume Portfolio AssignmentDocument1 paginăm100 Resume Portfolio Assignmentapi-283396653Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Chapter 101-160Document297 paginiChapter 101-160Dipankar BoruahÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- File 000011Document25 paginiFile 000011Jf LarongÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Phrygian Gates and China Gates RecordingsDocument1 paginăPhrygian Gates and China Gates RecordingsCloudwalkÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
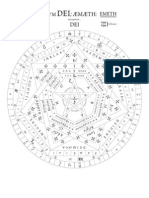
- John Dee - Sigillum Dei Aemeth or Seal of The Truth of God EnglishDocument2 paginiJohn Dee - Sigillum Dei Aemeth or Seal of The Truth of God Englishsatyr70286% (7)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Case Study 2022 - HeyJobsDocument6 paginiCase Study 2022 - HeyJobsericka.rolim8715Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Leverage My PptsDocument34 paginiLeverage My PptsMadhuram SharmaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Cyclosporin ARCDocument9 paginiCyclosporin ARCSean GreenÎncă nu există evaluări
- Week 1 Course Objectives and OutlineDocument15 paginiWeek 1 Course Objectives and Outlinechrisbourque13Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Exercise and Ppismp StudentsDocument6 paginiExercise and Ppismp StudentsLiyana RoseÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Investment Opportunities: Equity MarketsDocument38 paginiInvestment Opportunities: Equity MarketsRanjeet SinghÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Second Unit Test 2022: Radha Madhav Public School BareillyDocument4 paginiSecond Unit Test 2022: Radha Madhav Public School BareillyRaghav AgarwalÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Molina Vs de La Riva 6 Phil 12 INOKDocument2 paginiMolina Vs de La Riva 6 Phil 12 INOKErick Jay InokÎncă nu există evaluări
- Christian Education of Zendeling-Based at The Kalimantan Evangelical Church (GKE)Document16 paginiChristian Education of Zendeling-Based at The Kalimantan Evangelical Church (GKE)Editor IjrssÎncă nu există evaluări
- Unit 1session 2 Performance MGMTDocument38 paginiUnit 1session 2 Performance MGMTMayank TrivediÎncă nu există evaluări
- MahayanaDocument26 paginiMahayanaAleza Menorca100% (1)
- Blood Is A Body Fluid in Human and Other Animals That Delivers Necessary Substances Such AsDocument24 paginiBlood Is A Body Fluid in Human and Other Animals That Delivers Necessary Substances Such AsPaulo DanielÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Interpret Market Trends and Developments TASk 1Document7 paginiInterpret Market Trends and Developments TASk 1Raí SilveiraÎncă nu există evaluări
- EntropyDocument38 paginiEntropyPreshanth_Jaga_2224Încă nu există evaluări
- Invisible Rainbow A History of Electricity and LifeDocument17 paginiInvisible Rainbow A History of Electricity and LifeLarita Nievas100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Final For Influence of OJTDocument39 paginiFinal For Influence of OJTAnthony B. AnocheÎncă nu există evaluări
- Noorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester IDocument26 paginiNoorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester Iisaac RÎncă nu există evaluări
- Machine DesignDocument34 paginiMachine DesignMohammed Yunus33% (3)
- CR Injector Repair Kits 2016Document32 paginiCR Injector Repair Kits 2016Euro Diesel100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Product Design and DevelopmentDocument14 paginiProduct Design and Developmentajay3480100% (1)
- G.R. No. 205307 PEOPLE Vs EDUARDO GOLIDAN y COTO-ONGDocument24 paginiG.R. No. 205307 PEOPLE Vs EDUARDO GOLIDAN y COTO-ONGRuel FernandezÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)