S-ar putea să vă placă și
- Herbal Its Project Biology.....Document52 paginiHerbal Its Project Biology.....MISHAÎncă nu există evaluări
- Patient Details Date: Ref No: Address: PH No.:: Dr. Vanisha Mattu MbbsDocument1 paginăPatient Details Date: Ref No: Address: PH No.:: Dr. Vanisha Mattu MbbsrksjprÎncă nu există evaluări
- Al Ghazali and The SoulDocument7 paginiAl Ghazali and The SoulShafiq Mohamedtaqi100% (2)
- Al Ghazali and The SoulDocument7 paginiAl Ghazali and The SoulShafiq Mohamedtaqi100% (2)
- Seeking Divine Guidance IstikharaDocument10 paginiSeeking Divine Guidance IstikharaNorman AzriÎncă nu există evaluări
- GPAT and Gate Pharmacy 3rd Edition: GPAT and Gate Pharmacy 3rd EditionDe la EverandGPAT and Gate Pharmacy 3rd Edition: GPAT and Gate Pharmacy 3rd EditionEvaluare: 4.5 din 5 stele4.5/5 (6)
- Pharmacy Practice: Essentials of Hospital, Clinical and Community PharmacyDe la EverandPharmacy Practice: Essentials of Hospital, Clinical and Community PharmacyEvaluare: 5 din 5 stele5/5 (3)
- Ich-Gcp & Schedule yDocument38 paginiIch-Gcp & Schedule ySahiti PendyalaÎncă nu există evaluări
- Clinical WorkSheet - TemplateDocument23 paginiClinical WorkSheet - TemplateRene ContrerasÎncă nu există evaluări
- Stuart CloseDocument200 paginiStuart Closemihaipopescu0100% (1)
- Pharmacy and Therapeutics CommitteeDocument9 paginiPharmacy and Therapeutics CommitteeAl Sah HimÎncă nu există evaluări
- Al Mizan - Allamah Tabatabai Surah NisaDocument347 paginiAl Mizan - Allamah Tabatabai Surah NisaShafiq MohamedtaqiÎncă nu există evaluări
- Writing A Health Policy Brief With OutlineDocument14 paginiWriting A Health Policy Brief With OutlineyandhiasÎncă nu există evaluări
- RMH GP Referral: Service RequestedDocument2 paginiRMH GP Referral: Service RequestedHazem M. WardaÎncă nu există evaluări
- BC - Jurisprudence - FAQDocument7 paginiBC - Jurisprudence - FAQsanjayÎncă nu există evaluări
- Circular (24-2020) - EngDocument3 paginiCircular (24-2020) - EngdrnamithapedÎncă nu există evaluări
- Pharmaceutical Interview Form: One NameDocument85 paginiPharmaceutical Interview Form: One NameNirmal AliÎncă nu există evaluări
- Hypnotic and Anxiolytic Reduction or Withdrawal ResourcesDocument28 paginiHypnotic and Anxiolytic Reduction or Withdrawal ResourcesbarakaÎncă nu există evaluări
- Home Medication ReviewDocument31 paginiHome Medication ReviewFaiz MustaffaÎncă nu există evaluări
- English For Health Care ProvidersDocument7 paginiEnglish For Health Care ProvidersSusana MandyÎncă nu există evaluări
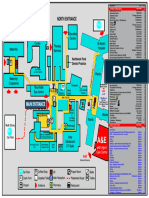
- Northwick Park Hospital Site MapDocument1 paginăNorthwick Park Hospital Site MapHasaan KhanÎncă nu există evaluări
- Soleclerkshiplong 2Document3 paginiSoleclerkshiplong 2Jovcel ObcenaÎncă nu există evaluări
- Our Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesDocument3 paginiOur Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesrenzÎncă nu există evaluări
- View PrescriptionDocument1 paginăView PrescriptionKancharana ManasaÎncă nu există evaluări
- The NDAC (Gastroenterology & Hepatology) NewDocument4 paginiThe NDAC (Gastroenterology & Hepatology) NewananthÎncă nu există evaluări
- Client Specific Non Formulary Drug Request FormDocument2 paginiClient Specific Non Formulary Drug Request FormNanaDinaWahyuniÎncă nu există evaluări
- Prescription Writing: Main Parts of A PrescriptionDocument5 paginiPrescription Writing: Main Parts of A PrescriptionJust AbdulElahÎncă nu există evaluări
- Handout On Prescription WritingDocument10 paginiHandout On Prescription WritingAbdiÎncă nu există evaluări
- GastroenterologyDocument2 paginiGastroenterologyPermis Pour Tous frÎncă nu există evaluări
- Ap PRCDocument31 paginiAp PRCvenkat yeluri100% (1)
- Dsip 2.4 BMX Mouthwash, Nitrofurantoin, OndansetronDocument17 paginiDsip 2.4 BMX Mouthwash, Nitrofurantoin, OndansetronGreatness AgwazeÎncă nu există evaluări
- Sample Station # 5 - Warfarin Carbamazepine InteractionDocument7 paginiSample Station # 5 - Warfarin Carbamazepine InteractionGregÎncă nu există evaluări
- ACFrOgApEAvt805mJBNhTdNTi2lw1XVIIRO9Hq53UAwNEdYxRDGfemdm8GE0OBiwvxQu1LywvZ11BnIh7 C PL3jinGyI2hzA K1yfdxe9n9BMDWap1kA SpIBoudZvTikzCFpNMYdVpryYuGnxwDocument1 paginăACFrOgApEAvt805mJBNhTdNTi2lw1XVIIRO9Hq53UAwNEdYxRDGfemdm8GE0OBiwvxQu1LywvZ11BnIh7 C PL3jinGyI2hzA K1yfdxe9n9BMDWap1kA SpIBoudZvTikzCFpNMYdVpryYuGnxwAbhishekÎncă nu există evaluări
- Chronic Medication For Other ConditionDocument5 paginiChronic Medication For Other ConditionGeorgeÎncă nu există evaluări
- HUKM PharmacyDocument2 paginiHUKM PharmacyLua Chiyar LockÎncă nu există evaluări
- Bma Prescribing in General Practice April 2018Document11 paginiBma Prescribing in General Practice April 2018Paulo'RodriguesÎncă nu există evaluări
- Bulletin Farmasi HPJ Bil 1 - 2015Document15 paginiBulletin Farmasi HPJ Bil 1 - 2015unionewÎncă nu există evaluări
- Medical Claim Form - FLEX StaffDocument1 paginăMedical Claim Form - FLEX StaffHerawaty Syaiful GusmentaÎncă nu există evaluări
- GP Management Plan - Mbs Item No. 721 (Asthma)Document3 paginiGP Management Plan - Mbs Item No. 721 (Asthma)Mohamed Rikarz Ahamed RikarzÎncă nu există evaluări
- 10 Day Use of Proton Pump Inhibitors in The Primary Care SettingDocument13 pagini10 Day Use of Proton Pump Inhibitors in The Primary Care Settingkarolina purbaÎncă nu există evaluări
- Discharge Summary Template 1Document1 paginăDischarge Summary Template 1Kitz Castillo-EnebradÎncă nu există evaluări
- List of Amhs AmasDocument11 paginiList of Amhs AmasNaveenkumar PalanisamyÎncă nu există evaluări
- Blank Discharge Summary TemplateDocument1 paginăBlank Discharge Summary Templatesujit shindeÎncă nu există evaluări
- Materi 3 Webinar Dit Standar BPOMDocument46 paginiMateri 3 Webinar Dit Standar BPOMtransitdokregÎncă nu există evaluări
- Mr. Ajit Kumar Singh 2 PDFDocument2 paginiMr. Ajit Kumar Singh 2 PDFajit kumar singhÎncă nu există evaluări
- Patient Details Ref No: Date & Time:: Dr. Poojitha Prasad MbbsDocument1 paginăPatient Details Ref No: Date & Time:: Dr. Poojitha Prasad Mbbssatyam goyalÎncă nu există evaluări
- Legislatie Retete AngliaDocument7 paginiLegislatie Retete AnglialatedayÎncă nu există evaluări
- MaxxDocument7 paginiMaxxmaverickmahendraÎncă nu există evaluări
- Activ Health Platinum Enhanced - One Pager - EnglishDocument2 paginiActiv Health Platinum Enhanced - One Pager - EnglishVARUNÎncă nu există evaluări
- ملف الشيماءDocument925 paginiملف الشيماءilyas khanÎncă nu există evaluări
- Monograph & PortfolioDocument33 paginiMonograph & PortfolioEph RemÎncă nu există evaluări
- Sample DMMR PlanDocument1 paginăSample DMMR PlanMIchelle SmithÎncă nu există evaluări
- Medication Passport: Clinical Site Student Please Complete Student Please Complete Context Please Date and SignDocument3 paginiMedication Passport: Clinical Site Student Please Complete Student Please Complete Context Please Date and SignGiselle GonzalezÎncă nu există evaluări
- Intervention Interdoc 2Document1 paginăIntervention Interdoc 2Marifuddin HussainiÎncă nu există evaluări
- Weekly Plan 04Document2 paginiWeekly Plan 04Nasir MahmoodÎncă nu există evaluări
- Disp 25 Hospital Flucloxacillin Cyclizine and Amiodarone NO COUNSELLING POINTS HEREDocument12 paginiDisp 25 Hospital Flucloxacillin Cyclizine and Amiodarone NO COUNSELLING POINTS HEREGreatness AgwazeÎncă nu există evaluări
- The Pharmacy & Therapeutic Committee Have Three Major Roles To PlayDocument14 paginiThe Pharmacy & Therapeutic Committee Have Three Major Roles To PlayPearlÎncă nu există evaluări
- PSB Requirements For Seeking Authorisation To Prescribe Ketamine For Treatment Resistant DepressionDocument6 paginiPSB Requirements For Seeking Authorisation To Prescribe Ketamine For Treatment Resistant DepressionandresÎncă nu există evaluări
- Government of West Bengal Department of Health and Family Welfare, Wing-A, 4 Floor, Swasthya Bhavan GN 29, Sector - V, Salt Lake, Kolkata - 700091Document33 paginiGovernment of West Bengal Department of Health and Family Welfare, Wing-A, 4 Floor, Swasthya Bhavan GN 29, Sector - V, Salt Lake, Kolkata - 700091meenakshi.r.agrawalÎncă nu există evaluări
- Reactive: Department of Chemical PathologyDocument1 paginăReactive: Department of Chemical PathologyHibaAliÎncă nu există evaluări
- Quetiapine IrDocument2 paginiQuetiapine IrChris SejÎncă nu există evaluări
- Inhaler Protocol Dec 2020Document2 paginiInhaler Protocol Dec 2020Sahira DarÎncă nu există evaluări
- Drug Study BipolarDocument13 paginiDrug Study BipolarrahimsyusophÎncă nu există evaluări
- FAQ MMA Borang JPJ L8ADocument1 paginăFAQ MMA Borang JPJ L8ATri Aero Sdn BhdÎncă nu există evaluări
- Respiratory System Medications Ventolin Peak Flow Meter 132300 2022 09 07 23 45 28Document5 paginiRespiratory System Medications Ventolin Peak Flow Meter 132300 2022 09 07 23 45 28Emad MustafaÎncă nu există evaluări
- Quick Reference DMARDsDocument12 paginiQuick Reference DMARDsEman MohamedÎncă nu există evaluări
- 17 June IPDocument13 pagini17 June IPraj_pegasusÎncă nu există evaluări
- CE CatalogDocument160 paginiCE CatalograchellycÎncă nu există evaluări
- Del Rosario v. BengzonDocument7 paginiDel Rosario v. BengzonLee YuÎncă nu există evaluări
- Timothy Healey Joins The Board of Director at Microvascular TherapeuticsDocument3 paginiTimothy Healey Joins The Board of Director at Microvascular TherapeuticsPR.comÎncă nu există evaluări
- Medical Surgical Nursing 9Th Edition Lewis Test Bank Full Chapter PDFDocument29 paginiMedical Surgical Nursing 9Th Edition Lewis Test Bank Full Chapter PDFsusan.dean734100% (12)
- Pharmacology Exam COHORT 8Document9 paginiPharmacology Exam COHORT 8Lesley Liavoga SandeÎncă nu există evaluări
- SUMMATIVE TEST in MAPEH 6Document11 paginiSUMMATIVE TEST in MAPEH 6Bezaleel JamesÎncă nu există evaluări
- Librium ChlordiazepoxideDocument2 paginiLibrium ChlordiazepoxideEÎncă nu există evaluări
- Patient Safety PDFDocument13 paginiPatient Safety PDFsnprianiÎncă nu există evaluări
- The Hip-Hop Issue No. 46Document37 paginiThe Hip-Hop Issue No. 46Edibles MagazineÎncă nu există evaluări
- ADRDocument34 paginiADRShaikh FaseehuddinÎncă nu există evaluări
- Emoderm CreamDocument4 paginiEmoderm CreamSM ZuhailÎncă nu există evaluări
- Egyptian Hospital Accreditation Program: Standards: Sixth Edition May 2005Document71 paginiEgyptian Hospital Accreditation Program: Standards: Sixth Edition May 2005khayisamÎncă nu există evaluări
- Modern Times Medicine Hepatitis C Suppliers-Exporters-Dealers India-Russia-ChinaDocument12 paginiModern Times Medicine Hepatitis C Suppliers-Exporters-Dealers India-Russia-ChinaKamal JindalÎncă nu există evaluări
- PCC Issues Paper 2020 02 A Profile of The Philippine Pharmaceutical IndustryDocument41 paginiPCC Issues Paper 2020 02 A Profile of The Philippine Pharmaceutical IndustryJoelle Faye Cortez100% (1)
- Prof. P. R. Vavia ResumeDocument50 paginiProf. P. R. Vavia ResumeGwen WalkerÎncă nu există evaluări
- 03 The Role of "Smart" Infusion Pumps in Patient Safety PDFDocument11 pagini03 The Role of "Smart" Infusion Pumps in Patient Safety PDFSaravanan NallasivanÎncă nu există evaluări
- RRL Anne)Document27 paginiRRL Anne)api-3728522Încă nu există evaluări
- Malaysian Pharmaceutical Industry: Opportunities and ChallengesDocument8 paginiMalaysian Pharmaceutical Industry: Opportunities and ChallengesChoko Ema SakuraÎncă nu există evaluări
- Tcs Life Sciences Whitepaper Pharma-Sales-MarketingDocument17 paginiTcs Life Sciences Whitepaper Pharma-Sales-Marketingbidump100% (1)
- Test Compilation PDFDocument25 paginiTest Compilation PDFAngelika VeluzÎncă nu există evaluări
- National Drug Policy 1995Document13 paginiNational Drug Policy 1995Madhu Sudhan PandeyaÎncă nu există evaluări
- ENGLISHDocument2 paginiENGLISHEmilia AndreiÎncă nu există evaluări
- Wallace State Community College NURSING DATABASE: Nursing HomeDocument9 paginiWallace State Community College NURSING DATABASE: Nursing HomeEnger NushunÎncă nu există evaluări
- A Study of The Use of Honey and Ethno-Biological Components in Nigerian Trado-Medical PracticesDocument12 paginiA Study of The Use of Honey and Ethno-Biological Components in Nigerian Trado-Medical PracticesRasco Damasta FuÎncă nu există evaluări
- RTIReport RemovingPriorAuthDocument14 paginiRTIReport RemovingPriorAuthBethanyÎncă nu există evaluări
- Relevance of Rasa Shastra in 21St Century With Special Reference To Lifestyle Disorders (LSDS)Document6 paginiRelevance of Rasa Shastra in 21St Century With Special Reference To Lifestyle Disorders (LSDS)Payal Is LearningÎncă nu există evaluări
- Food - Drug InteractionsDocument36 paginiFood - Drug InteractionsDr-ir Faisal HasanÎncă nu există evaluări