S-ar putea să vă placă și
- Visual-Motor Skills Test for ChildrenDocument6 paginiVisual-Motor Skills Test for ChildrenAmine Venta100% (2)
- OT Appendix Tables-Mar.2006Document12 paginiOT Appendix Tables-Mar.2006Yas DGÎncă nu există evaluări
- M-FUN Assessment ReviewDocument4 paginiM-FUN Assessment ReviewKishan RamtohulÎncă nu există evaluări
- Vmi PresentationDocument31 paginiVmi Presentationapi-311896275100% (3)
- Salhi Beery Vmi Write UpDocument4 paginiSalhi Beery Vmi Write Upapi-547482419Încă nu există evaluări
- Beery VMI 5-Ed Assessment ReviewDocument4 paginiBeery VMI 5-Ed Assessment ReviewMilena Almeida75% (8)
- BOTMP2Document31 paginiBOTMP2蘇永泓Încă nu există evaluări
- Pediatric Evaluation ReportDocument3 paginiPediatric Evaluation Reportapi-469965619Încă nu există evaluări
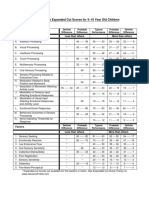
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 paginăSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliÎncă nu există evaluări
- BOT 2 Webinar Handout 092115Document23 paginiBOT 2 Webinar Handout 092115Mikey PanupongÎncă nu există evaluări
- Sensory ProfileDocument8 paginiSensory ProfilenymommyÎncă nu există evaluări
- Handwriting Speed Assessment Pa TossDocument4 paginiHandwriting Speed Assessment Pa Tossdeni44450% (4)
- BOT-2 Fine Motor Assessment GuideDocument17 paginiBOT-2 Fine Motor Assessment GuideVictor Bravo OlivaresÎncă nu există evaluări
- Beery VMIDocument10 paginiBeery VMISteffiDoankSih50% (2)
- Ot Assessment Template - SelpaDocument5 paginiOt Assessment Template - Selpaapi-417867603100% (1)
- Ot Guidelines Child SpecificDocument34 paginiOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Sfa Scool Function AssementDocument18 paginiSfa Scool Function AssementAnielle OliveiraÎncă nu există evaluări
- PEDI CAT Manual 1 3 6 PDFDocument162 paginiPEDI CAT Manual 1 3 6 PDFSari Nm100% (2)
- Sensory ProfileDocument5 paginiSensory ProfileNika GarciaÎncă nu există evaluări
- Double Time Docs Sample Evaluation OT SchoolDocument10 paginiDouble Time Docs Sample Evaluation OT SchoolAlyssa Balverde100% (1)
- Bayley ScalesDocument7 paginiBayley Scalesmrabhilekh100% (1)
- CO OP AOTA - July - 2020Document10 paginiCO OP AOTA - July - 2020Ana Claudia GomesÎncă nu există evaluări
- GMFMscoresheetDocument6 paginiGMFMscoresheetAbdur RasyidÎncă nu există evaluări
- School Function AssessmentDocument8 paginiSchool Function AssessmentPaulina Vergara67% (3)
- Motor Assessments For School Aged Children and AdolescentsDocument17 paginiMotor Assessments For School Aged Children and AdolescentsdelfiaÎncă nu există evaluări
- BSID ASSESSMENTDocument6 paginiBSID ASSESSMENTRabab Ruby NullwalaÎncă nu există evaluări
- Sensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'AmDocument42 paginiSensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'Amamandeep kaurÎncă nu există evaluări
- SPM P 3 5 Anos Home PDFDocument2 paginiSPM P 3 5 Anos Home PDFkateb dienelÎncă nu există evaluări
- Ot Goals NuevoDocument157 paginiOt Goals NuevoElbania PerezÎncă nu există evaluări
- Senior Occupational Therapist: Passbooks Study GuideDe la EverandSenior Occupational Therapist: Passbooks Study GuideÎncă nu există evaluări
- SPM Manual Chapter 1Document4 paginiSPM Manual Chapter 1Jairo Andres Chavarria Alvarado20% (5)
- Occupation Analysis in PracticeDe la EverandOccupation Analysis in PracticeLynette MackenzieÎncă nu există evaluări
- Bayley-III Clinical Use and InterpretationDe la EverandBayley-III Clinical Use and InterpretationEvaluare: 2 din 5 stele2/5 (1)
- Teste VmiDocument21 paginiTeste VmiFlahiza Marques100% (3)
- Student Treatment Session Soap 8Document9 paginiStudent Treatment Session Soap 8api-340625860100% (1)
- Building Blocks for Learning Occupational Therapy Approaches: Practical Strategies for the Inclusion of Special Needs in Primary SchoolDe la EverandBuilding Blocks for Learning Occupational Therapy Approaches: Practical Strategies for the Inclusion of Special Needs in Primary SchoolÎncă nu există evaluări
- BOT-2 Complete Form Sample ReportDocument12 paginiBOT-2 Complete Form Sample Reportkonna4539100% (3)
- Bayley Scales of DevelopmentDocument14 paginiBayley Scales of Developmenttrcoski100% (3)
- Soap Notes Dot Phrases For Occupational TherapistsDe la EverandSoap Notes Dot Phrases For Occupational TherapistsÎncă nu există evaluări
- Caregiver Sensory ProfileDocument6 paginiCaregiver Sensory ProfileRomysah Farooq100% (1)
- COSA Summary FormDocument2 paginiCOSA Summary FormSara CostaÎncă nu există evaluări
- Pediatric Disorders of Regulation in Affect and Behavior: A Therapist's Guide to Assessment and TreatmentDe la EverandPediatric Disorders of Regulation in Affect and Behavior: A Therapist's Guide to Assessment and TreatmentEvaluare: 5 din 5 stele5/5 (2)
- Basc 3 Rating Scales SampleDocument28 paginiBasc 3 Rating Scales SampleMohammed Abu shawish100% (1)
- Clinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Document16 paginiClinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Jhon Liev100% (2)
- BOT-2 Complete Form Sample Report PDFDocument12 paginiBOT-2 Complete Form Sample Report PDFmarioh_40% (1)
- Neurological Assessment in the First Two Years of LifeDe la EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniÎncă nu există evaluări
- Space Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDocument4 paginiSpace Management: 0 To 6 Months 6 To 12 Months 12 To 18 MonthsDaNelle McPhaddenÎncă nu există evaluări
- Binocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/ADe la EverandBinocular Saccadic Dysfunction - a Precursor to Dyslexia?: N/AÎncă nu există evaluări
- Cosa Manual 1Document103 paginiCosa Manual 1clara100% (2)
- Fine Motor and Handwriting Skills ActivitiesDocument4 paginiFine Motor and Handwriting Skills Activitiesehopkins5_209Încă nu există evaluări
- BriganceDocument1 paginăBriganceamf780% (1)
- Using The Infant/Toddler Sensory Profile in Early Intervention ServicesDocument65 paginiUsing The Infant/Toddler Sensory Profile in Early Intervention Servicesfitomena50% (2)
- Portage Guide To Early EducationDocument18 paginiPortage Guide To Early EducationSaman Khan100% (4)
- Occupational Therapy Assessment ToolsDocument19 paginiOccupational Therapy Assessment ToolsThirdy BullerÎncă nu există evaluări
- GMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionDe la EverandGMFM (GMFM-66 & GMFM-88) User's Manual, 2nd editionÎncă nu există evaluări
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionDe la EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionÎncă nu există evaluări
- MINONGADocument5 paginiMINONGALeslie100% (3)
- Dana Saville ArtDocument1 paginăDana Saville ArtDana SavilleÎncă nu există evaluări
- Xie Boush 2011Document22 paginiXie Boush 2011ark3003Încă nu există evaluări
- Leisure Time To The Academic of StudentDocument12 paginiLeisure Time To The Academic of StudentKate Tolentino Macalintal0% (1)
- Additional ProblemDocument3 paginiAdditional ProblemthanhvanngocphamÎncă nu există evaluări
- Surgery Mind MapDocument4 paginiSurgery Mind MapioakasÎncă nu există evaluări
- Final Year Project Examination Time TableDocument7 paginiFinal Year Project Examination Time TableVid YashaÎncă nu există evaluări
- Lecture-2.1.6Document13 paginiLecture-2.1.6gdgdÎncă nu există evaluări
- Intro. To Philo. Q2 (Module2)Document8 paginiIntro. To Philo. Q2 (Module2)Bernie P. RamaylaÎncă nu există evaluări
- Indian states with highest and lowest dropout ratesDocument23 paginiIndian states with highest and lowest dropout ratesAJIT SINGHÎncă nu există evaluări
- Materials Adaptation of Eap Materials - Part 2Document6 paginiMaterials Adaptation of Eap Materials - Part 2api-402780610Încă nu există evaluări
- OutLines of European Board Exam-HNS - ExamDocument19 paginiOutLines of European Board Exam-HNS - ExamDrMohmd ZidaanÎncă nu există evaluări
- Hemangioma Guide for DoctorsDocument29 paginiHemangioma Guide for DoctorshafiizhdpÎncă nu există evaluări
- Morning Sleepiness Among College Students: Surprising Reasons For Class-Time PreferenceDocument4 paginiMorning Sleepiness Among College Students: Surprising Reasons For Class-Time PreferenceElijah NyakundiÎncă nu există evaluări
- Annotated BibliographyDocument3 paginiAnnotated Bibliographyapi-406951522Încă nu există evaluări
- Chief Petron: Dr. Bankim R. ThakarDocument2 paginiChief Petron: Dr. Bankim R. Thakargoswami vaishalÎncă nu există evaluări
- Become An Aviation Mechanic - FAADocument14 paginiBecome An Aviation Mechanic - FAAPanagiotis AlexandrisÎncă nu există evaluări
- Cognitive Components of Social AnxietyDocument4 paginiCognitive Components of Social AnxietyAdina IlieÎncă nu există evaluări
- Part 6 Uasa Short Communicative Message - 1Document4 paginiPart 6 Uasa Short Communicative Message - 1Pearlyn LoÎncă nu există evaluări
- Textbox 1 1 1Document3 paginiTextbox 1 1 1api-200842148Încă nu există evaluări
- Audio/Radio Production I Syllabus: Dallas College North Lake CampusDocument13 paginiAudio/Radio Production I Syllabus: Dallas College North Lake CampusUriel MenesesÎncă nu există evaluări
- Child and Adolescent DevelopmentDocument5 paginiChild and Adolescent Developmentandrew gauranaÎncă nu există evaluări
- Sci GDocument12 paginiSci GEvans KipyegoÎncă nu există evaluări
- Unit 2 Test B Listening, Language, Reading, Communication SkillsDocument2 paginiUnit 2 Test B Listening, Language, Reading, Communication SkillsAnia YemelyanovaÎncă nu există evaluări
- Instrument Music Lesson Plan: KindergartenDocument4 paginiInstrument Music Lesson Plan: Kindergartenapi-510351548Încă nu există evaluări
- UTSCCalendar2014 2015Document389 paginiUTSCCalendar2014 2015islandemiajÎncă nu există evaluări
- Residential Comprehensive 2015 Leaflet PDFDocument7 paginiResidential Comprehensive 2015 Leaflet PDFmsatpathy2003Încă nu există evaluări
- 43 All India Conference of Dravidian LinguistsDocument6 pagini43 All India Conference of Dravidian LinguistsV N BHATTATHIRIÎncă nu există evaluări
- Pitagan discusses media, eLearning, 21st century learningDocument34 paginiPitagan discusses media, eLearning, 21st century learningReymond CuisonÎncă nu există evaluări
- CTFL 2018 Sample Exam B v1.3 QuestionsDocument21 paginiCTFL 2018 Sample Exam B v1.3 QuestionsLaser- xÎncă nu există evaluări