S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Antibodies A Laboratory Manual Edited byDocument1 paginăAntibodies A Laboratory Manual Edited by廖詠凝Încă nu există evaluări
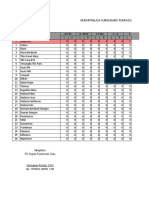
- Laporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuDocument37 paginiLaporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuVictoria YanersÎncă nu există evaluări
- Day 36 - Daily MCQ Workout - 40 Revision MCQsDocument6 paginiDay 36 - Daily MCQ Workout - 40 Revision MCQsnorah araujoÎncă nu există evaluări
- Patient Blepharitis LeafletDocument2 paginiPatient Blepharitis LeafletPrincess ErickaÎncă nu există evaluări
- Swab GuideDocument1 paginăSwab GuideMoe Zaw LinÎncă nu există evaluări
- 10 Larva MigransDocument8 pagini10 Larva MigransDaniel JohnsonÎncă nu există evaluări
- Gajdos 2015Document9 paginiGajdos 2015Rafa NaufalinÎncă nu există evaluări
- Immunology FirecrackerDocument45 paginiImmunology FirecrackerMariam A. KarimÎncă nu există evaluări
- AIDS in Pre-AIDS EraDocument7 paginiAIDS in Pre-AIDS EraObginÎncă nu există evaluări
- Unwell Child PosterDocument2 paginiUnwell Child PosterGabriella GriffithsÎncă nu există evaluări
- Complete Protein Antigens and Low - Molecular-Weight Substances - Complete Protein Antigens, Such As AnimalDocument1 paginăComplete Protein Antigens and Low - Molecular-Weight Substances - Complete Protein Antigens, Such As AnimalApple BananaÎncă nu există evaluări
- Asthma - PROF WASEEM (2022)Document36 paginiAsthma - PROF WASEEM (2022)Mahnoor AyeshaÎncă nu există evaluări
- ABO Blood Group System NotesDocument45 paginiABO Blood Group System NotesAnne Carmel Verano100% (1)
- Microbiology 1st Semeter BSN Mcqs by RCN, Educational PlatformDocument10 paginiMicrobiology 1st Semeter BSN Mcqs by RCN, Educational PlatformPrince Masroor Ali AbroÎncă nu există evaluări
- National Immunisation Program Schedule Landscape National Immunisation Program Childhood Schedule Changes Schedule Card Landscape - 0Document1 paginăNational Immunisation Program Schedule Landscape National Immunisation Program Childhood Schedule Changes Schedule Card Landscape - 0Samreet SinghÎncă nu există evaluări
- Atopic Dermatitis: Skin-Directed Management: Clinical ReportDocument12 paginiAtopic Dermatitis: Skin-Directed Management: Clinical ReportDenia Haritsa AprilianiÎncă nu există evaluări
- CHICKENPOXDocument36 paginiCHICKENPOXAlyssa Marie Pepito100% (1)
- 1991 - de Groot Et Al. - Affinity Purification of A Major and A Minor Allergen From Dog Extract Serologic Activity of Affinity-Purified CanDocument10 pagini1991 - de Groot Et Al. - Affinity Purification of A Major and A Minor Allergen From Dog Extract Serologic Activity of Affinity-Purified Canpond_1993Încă nu există evaluări
- c-ANCA ELISADocument2 paginic-ANCA ELISAYousra ZeidanÎncă nu există evaluări
- Girl Scouts of The Philippines PermitDocument1 paginăGirl Scouts of The Philippines Permitbrave29heartÎncă nu există evaluări
- Platelet Disorders ItpDocument13 paginiPlatelet Disorders ItpWadood Saeed100% (1)
- Bacterial InfectionDocument41 paginiBacterial InfectionUmmi Rinandari100% (1)
- Heather Zwickey, PHD - Important Clarifications Regarding Covid-19 and Natural Medicine - Dispelling Myths and MisconceptionsDocument9 paginiHeather Zwickey, PHD - Important Clarifications Regarding Covid-19 and Natural Medicine - Dispelling Myths and Misconceptionstahuti696Încă nu există evaluări
- Onsite: Hsv-2 Igg/Igm Rapid TestDocument2 paginiOnsite: Hsv-2 Igg/Igm Rapid TestsafiraplÎncă nu există evaluări
- ArticleDocument8 paginiArticleIonescu Raluca VioletaÎncă nu există evaluări
- Poster Sesion 3Document120 paginiPoster Sesion 3Javierf EstaritaguerreroÎncă nu există evaluări
- Diagnosis and Management of Polytraumatized.1Document6 paginiDiagnosis and Management of Polytraumatized.1María José Bueno MonteroÎncă nu există evaluări
- Necrotizing FasciitisDocument5 paginiNecrotizing Fasciitisnsl1225Încă nu există evaluări
- Anti-HBc IgM ElisaDocument20 paginiAnti-HBc IgM ElisaValia Condori JoveÎncă nu există evaluări
- Experiment #4: Demonstration of Common Immunohematologic ReactionsDocument5 paginiExperiment #4: Demonstration of Common Immunohematologic ReactionsKriziaÎncă nu există evaluări