S-ar putea să vă placă și
- Human VoiceDocument9 paginiHuman VoiceAurora SeasonÎncă nu există evaluări
- Nose Short NoteDocument163 paginiNose Short NoteAimanÎncă nu există evaluări
- Complications in Endoscopic Sinus Surgery - Diagnosis, Prevention and Management 2nd EditionDocument241 paginiComplications in Endoscopic Sinus Surgery - Diagnosis, Prevention and Management 2nd EditionRahat tanvirÎncă nu există evaluări
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument22 paginiMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El HageÎncă nu există evaluări
- Approaches To Frontal SinusDocument77 paginiApproaches To Frontal SinusHossam Elden Helmy HaridyÎncă nu există evaluări
- Anatomy and Evaluation in RhinoplastyDocument20 paginiAnatomy and Evaluation in RhinoplastyLaureano FilhoÎncă nu există evaluări
- Endoscopic Anatomy of Nose and PNS FinalDocument98 paginiEndoscopic Anatomy of Nose and PNS FinalRahul Kurkure100% (2)
- Lateral Wall of NoseDocument61 paginiLateral Wall of NoseMohammed Riyas100% (4)
- CT PNSDocument22 paginiCT PNSHany85Încă nu există evaluări
- Atlas of Paranasal Sinus SurgeryDocument81 paginiAtlas of Paranasal Sinus SurgeryNemer Al-KhtoumÎncă nu există evaluări
- Basic FESS - Step-By-Step Guide With Surgical Videos PDFDocument20 paginiBasic FESS - Step-By-Step Guide With Surgical Videos PDFMujeeb MohammedÎncă nu există evaluări
- CT Scan Variation SinusDocument67 paginiCT Scan Variation SinusDwi Utari PratiwiÎncă nu există evaluări
- Occluion ConceptsDocument15 paginiOccluion ConceptsImran CassimÎncă nu există evaluări
- Sinonasal Imaging PDFDocument17 paginiSinonasal Imaging PDFBelanny DwiÎncă nu există evaluări
- Cephalometric Evaluation and Measurement of The Upper Airway PDFDocument13 paginiCephalometric Evaluation and Measurement of The Upper Airway PDFSoe San KyawÎncă nu există evaluări
- Colour Atlas of The Anatomy and Pathology of The EpitympanumDocument110 paginiColour Atlas of The Anatomy and Pathology of The Epitympanumapi-26081450Încă nu există evaluări
- Endoscopic Surgery of The Lateral Nasal Wall, Paranasal Sinuses, and Anterior Skull Base (PDFDrive)Document268 paginiEndoscopic Surgery of The Lateral Nasal Wall, Paranasal Sinuses, and Anterior Skull Base (PDFDrive)Butt KÎncă nu există evaluări
- Cleft Lip and Palate Management: A Comprehensive AtlasDe la EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunÎncă nu există evaluări
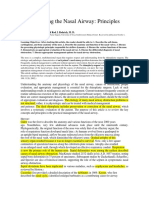
- Understanding The Nasal AirwayDocument21 paginiUnderstanding The Nasal AirwayGera AguilarÎncă nu există evaluări
- Oleson2014-Auricle Accupuncture NomenclatureDocument15 paginiOleson2014-Auricle Accupuncture NomenclaturebillÎncă nu există evaluări
- Understanding The Nasal Airway COLABORATIVODocument25 paginiUnderstanding The Nasal Airway COLABORATIVOCristal SerranoÎncă nu există evaluări
- 10 1 1 553 7658 PDFDocument6 pagini10 1 1 553 7658 PDFAgustino IdongÎncă nu există evaluări
- Oral Exostoses: An Assessment of Two Hundred Years of Research Les Exostoses Orales: Bilan de Deux Siècles de RecherchesDocument22 paginiOral Exostoses: An Assessment of Two Hundred Years of Research Les Exostoses Orales: Bilan de Deux Siècles de RecherchesYusuf DiansyahÎncă nu există evaluări
- He International Frontal Sinus Anatomy Classification (IFAC) and Classification of The Extent of Endoscopic Frontal Sinus Surgery (EFSSDocument20 paginiHe International Frontal Sinus Anatomy Classification (IFAC) and Classification of The Extent of Endoscopic Frontal Sinus Surgery (EFSSanitaabreu123Încă nu există evaluări
- 4 Nose and PhiltrumDocument16 pagini4 Nose and PhiltrumJessica Lissette CadilloÎncă nu există evaluări
- Lobes, Fissures, and Bronchopulmonary SegmentsDocument13 paginiLobes, Fissures, and Bronchopulmonary SegmentsJansi OrtizÎncă nu există evaluări
- NewTerminologiaAnatomicahighlightstheimportanceofclinicalanatomy PDFDocument13 paginiNewTerminologiaAnatomicahighlightstheimportanceofclinicalanatomy PDFanishaÎncă nu există evaluări
- Frontal Sinus and Frontal RecessDocument12 paginiFrontal Sinus and Frontal Recesspunct_org3256Încă nu există evaluări
- Apsm 2017 17 4 (1) 54Document3 paginiApsm 2017 17 4 (1) 54bose_lowe11Încă nu există evaluări
- Upper Nasal AirwayDocument23 paginiUpper Nasal AirwayKapil ThakerÎncă nu există evaluări
- Anatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsDocument24 paginiAnatomical Classification of Facial, Cranio-Facial and Latero-Facial CleftsAlvaro Jose Uribe TamaraÎncă nu există evaluări
- Metopism and Its Correlation With The Development of The Frontal SinusesDocument11 paginiMetopism and Its Correlation With The Development of The Frontal SinusesSorin-Valentin MocanuÎncă nu există evaluări
- Magnification and IlluminationDocument22 paginiMagnification and Illuminationwhussien7376100% (1)
- Anatomy and Development of Oral Cavity and PharynxDocument14 paginiAnatomy and Development of Oral Cavity and PharynxGabriela MacoveanuÎncă nu există evaluări
- Rhinoscopyinthedog1 AnatomyandtechniquesDocument8 paginiRhinoscopyinthedog1 AnatomyandtechniquesZackiary YukiÎncă nu există evaluări
- Fascial Nomenclature: Update On Related Consensus ProcessDocument5 paginiFascial Nomenclature: Update On Related Consensus ProcessPedro MouraÎncă nu există evaluări
- Modular Facial DisassemblyDocument7 paginiModular Facial DisassemblyKrithika AcÎncă nu există evaluări
- A Intubarion DownloadDocument8 paginiA Intubarion DownloadDiegoÎncă nu există evaluări
- Molluscan Studies: Journal ofDocument19 paginiMolluscan Studies: Journal ofWidi SetyogatiÎncă nu există evaluări
- Fascial Nomenclature Update On Related CDocument5 paginiFascial Nomenclature Update On Related Chppp555Încă nu există evaluări
- Mastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFDocument5 paginiMastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFPutu Reza Sandhya PratamaÎncă nu există evaluări
- New Perspectives On The Surgical Anatomy and Nomenclature of Temporal Region (2013)Document14 paginiNew Perspectives On The Surgical Anatomy and Nomenclature of Temporal Region (2013)enzoÎncă nu există evaluări
- 2015 KlugHoffmann AmmonoidSepta 3Document47 pagini2015 KlugHoffmann AmmonoidSepta 3Rafael Roldán de la RúaÎncă nu există evaluări
- Deposition, Clearance, and Translocation of Chrysotile Asbestos From Peripheral and Central Regions of The Rat LungDocument20 paginiDeposition, Clearance, and Translocation of Chrysotile Asbestos From Peripheral and Central Regions of The Rat LungKhambang AirlanggaÎncă nu există evaluări
- Comprehensive and Clinical Anatomy of the Middle EarDe la EverandComprehensive and Clinical Anatomy of the Middle EarÎncă nu există evaluări
- 16 Clinically Significant Variation of Paranasal Sinuses On CT ScanDocument6 pagini16 Clinically Significant Variation of Paranasal Sinuses On CT ScanAjeng Salsabila PawestriÎncă nu există evaluări
- Methods of Voice ReconstructionDocument7 paginiMethods of Voice Reconstructionalison quahÎncă nu există evaluări
- Collett 1993Document6 paginiCollett 1993SEBASTIAN ANDRES MIRANDA GONZALEZÎncă nu există evaluări
- The Nasal Septum PDFDocument18 paginiThe Nasal Septum PDFalit100% (1)
- History of Anaesthesia Oropharyngeal and Nasopharyngeal Airways: I (1880-1995)Document7 paginiHistory of Anaesthesia Oropharyngeal and Nasopharyngeal Airways: I (1880-1995)Lucille IlaganÎncă nu există evaluări
- Median (Third) Occipital CondyleDocument4 paginiMedian (Third) Occipital Condylespin_echoÎncă nu există evaluări
- (10920684 - Neurosurgical Focus) The Dorello Canal: Historical Development, Controversies in Microsurgical Anatomy, and Clinical ImplicationsDocument7 pagini(10920684 - Neurosurgical Focus) The Dorello Canal: Historical Development, Controversies in Microsurgical Anatomy, and Clinical ImplicationsKeng-Liang KuoÎncă nu există evaluări
- The Relationships Between Craniofacial Structure and Frontal Sinus Morphology: Evaluation With Conventional Anthropometry and CT-Based VolumetryDocument11 paginiThe Relationships Between Craniofacial Structure and Frontal Sinus Morphology: Evaluation With Conventional Anthropometry and CT-Based VolumetryfebriÎncă nu există evaluări
- Bankier Et Al 2024 Fleischner Society Glossary of Terms For Thoracic ImagingDocument55 paginiBankier Et Al 2024 Fleischner Society Glossary of Terms For Thoracic ImagingAna CamachoÎncă nu există evaluări
- California State Journal 1904 173: Some Recent Advances andDocument2 paginiCalifornia State Journal 1904 173: Some Recent Advances andAbdurRahmanÎncă nu există evaluări
- Radiologic History Exhibit Musculoskeletal EponymsDocument19 paginiRadiologic History Exhibit Musculoskeletal EponymsSangeetha KumariÎncă nu există evaluări
- Craniofacial Morphology of Wind and String Instrument Players: A Cephalometric Study.Document9 paginiCraniofacial Morphology of Wind and String Instrument Players: A Cephalometric Study.APinhaoFerreiraÎncă nu există evaluări
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 paginiVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123Încă nu există evaluări
- Ultrasound - of - The - Airway Paper3Document7 paginiUltrasound - of - The - Airway Paper3Indhu SubbuÎncă nu există evaluări
- Effects of Rapid Maxillary Expansion With A Memory Palatal Split Screw On The Morphology of The Maxillary Dental Arch and Nasal Airway ResistanceDocument5 paginiEffects of Rapid Maxillary Expansion With A Memory Palatal Split Screw On The Morphology of The Maxillary Dental Arch and Nasal Airway ResistanceMariana SantosÎncă nu există evaluări
- Rapid Maxillary ExpansionDocument55 paginiRapid Maxillary ExpansionDon George GeojanÎncă nu există evaluări
- Skeleton System of CattleDocument19 paginiSkeleton System of CattleRaluca Șerboiu0% (1)
- Preserving Oral Communication in Individuals With Tracheostomy and Ventilator DenpendencyDocument7 paginiPreserving Oral Communication in Individuals With Tracheostomy and Ventilator Denpendencypico 24Încă nu există evaluări
- Bilateral Nasolabial Cyst MarcoviceanuDocument4 paginiBilateral Nasolabial Cyst MarcoviceanubamsusiloÎncă nu există evaluări
- Third Molar Surgery: Past, Present, and The Future: Statement of Clinical RelevanceDocument9 paginiThird Molar Surgery: Past, Present, and The Future: Statement of Clinical RelevanceJean Carlos Barbosa FerreiraÎncă nu există evaluări
- The Temporomandibular Joint: Pneumatic Temporal Cells Open Into The Articular and Extradural SpacesDocument7 paginiThe Temporomandibular Joint: Pneumatic Temporal Cells Open Into The Articular and Extradural SpacesBs PhuocÎncă nu există evaluări
- Buccal Fat PadDocument21 paginiBuccal Fat PadPranave PÎncă nu există evaluări
- Embryology of Oesophageal Atresia: Adonis S. Ioannides, Andrew J. CoppDocument10 paginiEmbryology of Oesophageal Atresia: Adonis S. Ioannides, Andrew J. CoppXimenita GhilardiÎncă nu există evaluări
- Mikami 1987Document4 paginiMikami 1987Carlos CahuayaÎncă nu există evaluări
- Tooth Position in Wind Instrument Players: Dentofacial Cephalometric AnalysisDocument22 paginiTooth Position in Wind Instrument Players: Dentofacial Cephalometric AnalysisMauricio FemeniaÎncă nu există evaluări
- Endoscopic Ethmoidectomy - FESS - Surgical TechniqueDocument30 paginiEndoscopic Ethmoidectomy - FESS - Surgical TechniqueSaurav GurungÎncă nu există evaluări
- Endoscopic Ethmoidectomy - FESS - Surgical TechniqueDocument29 paginiEndoscopic Ethmoidectomy - FESS - Surgical TechniquekityamuwesiÎncă nu există evaluări
- Paranasal Sinuses - Anatomlc Termlnology and NomenclatureDocument10 paginiParanasal Sinuses - Anatomlc Termlnology and NomenclatureMaleus IncusÎncă nu există evaluări
- Ecr2017 C-2117Document66 paginiEcr2017 C-2117Ezekiel ArtetaÎncă nu există evaluări
- CT of The Paranasal Sinuses Normal Anatomyvariants and PathologyDocument10 paginiCT of The Paranasal Sinuses Normal Anatomyvariants and PathologyAndi FirdaÎncă nu există evaluări
- 3 Nose - Paranasal Sinus (More Modified)Document28 pagini3 Nose - Paranasal Sinus (More Modified)adham bani younesÎncă nu există evaluări
- Anatomy of Nose and PNS Final-1Document132 paginiAnatomy of Nose and PNS Final-1Sangam AdhikariÎncă nu există evaluări
- CT Scan Sinus ParanasalDocument21 paginiCT Scan Sinus ParanasalDewi BoedhiyonoÎncă nu există evaluări
- Anatomy and Physiology of The Nose and Paranasal Sinuses. Diagnosis and Management of RhinosinusitisDocument87 paginiAnatomy and Physiology of The Nose and Paranasal Sinuses. Diagnosis and Management of RhinosinusitisDanielicah Cruz100% (1)
- Sarad Chandra RevisionDocument18 paginiSarad Chandra RevisionPrabhat KcÎncă nu există evaluări
- Paranasal Sinus AnatomyDocument35 paginiParanasal Sinus AnatomyGeorge DaviesÎncă nu există evaluări
- Paranasal Sinus (Repaired) EntDocument48 paginiParanasal Sinus (Repaired) EntDr-Firas Nayf Al-ThawabiaÎncă nu există evaluări
- Vertebral Column Skull Projection MethodDocument8 paginiVertebral Column Skull Projection MethodLaFranz CabotajeÎncă nu există evaluări
- Viva NotesDocument210 paginiViva NotesIsaac Tan Yieng LerÎncă nu există evaluări
- Ent Rajeev Dhawan Full NotesDocument80 paginiEnt Rajeev Dhawan Full Notesrandomuploader053Încă nu există evaluări
- CD PNSsDocument87 paginiCD PNSsNan EarmworasinÎncă nu există evaluări
- 2021, Anatomical Factors That Can Predict The Structure of Lamina Papyracea For Endoscopic Sinus SurgeryDocument8 pagini2021, Anatomical Factors That Can Predict The Structure of Lamina Papyracea For Endoscopic Sinus SurgerycaromoradÎncă nu există evaluări
- Paranasal Sinus Anatomy - Overview, Gross Anatomy, Microscopic AnatomyDocument12 paginiParanasal Sinus Anatomy - Overview, Gross Anatomy, Microscopic AnatomyKienlevy100% (1)