S-ar putea să vă placă și
- Opium in BritianDocument23 paginiOpium in BritianRobert Clark100% (1)
- Medical History 19th CenturyDocument43 paginiMedical History 19th CenturyRobert ClarkÎncă nu există evaluări
- Oscar WildeDocument1 paginăOscar WildeRobert ClarkÎncă nu există evaluări
- Narcotic TreatmntdirDocument228 paginiNarcotic TreatmntdirRobert ClarkÎncă nu există evaluări
- Heroin FactsDocument6 paginiHeroin FactsRobert ClarkÎncă nu există evaluări
- Heroin Main Tan Ace NewEnglandournalJMedicine2009Document2 paginiHeroin Main Tan Ace NewEnglandournalJMedicine2009Robert ClarkÎncă nu există evaluări
- Heroin Maintance FactsSALOME FAQs v4Document6 paginiHeroin Maintance FactsSALOME FAQs v4Robert ClarkÎncă nu există evaluări
- Report To Congressional Requesters: United States Government Accountability OfficeDocument55 paginiReport To Congressional Requesters: United States Government Accountability OfficeRobert ClarkÎncă nu există evaluări
- Heroin Main Tan Ace FactsDocument20 paginiHeroin Main Tan Ace FactsRobert ClarkÎncă nu există evaluări
- Benzodiazepines: How They Work and How To Withdraw: (Aka The Ashton Manual)Document11 paginiBenzodiazepines: How They Work and How To Withdraw: (Aka The Ashton Manual)Ahmad Ulil AlbabÎncă nu există evaluări
- NarcoticsDocument9 paginiNarcoticsRobert ClarkÎncă nu există evaluări
- Drug History BritianDocument14 paginiDrug History BritianRobert ClarkÎncă nu există evaluări
- Harrison Narcotics ACT 1917Document6 paginiHarrison Narcotics ACT 1917Robert ClarkÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
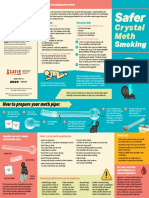
- CATIE SaferSmoking CrystalMeth E 2020 FINAL WEBDocument2 paginiCATIE SaferSmoking CrystalMeth E 2020 FINAL WEBJeff PuglisiÎncă nu există evaluări
- 7.-Naloxone-Administration-Training-PowerPoint 2Document19 pagini7.-Naloxone-Administration-Training-PowerPoint 2Ariesta Nurfitria KhansaÎncă nu există evaluări
- Naloxone in AdultsDocument8 paginiNaloxone in AdultsRoboschi StefaniaÎncă nu există evaluări
- Opioid Reduction Act SummaryDocument2 paginiOpioid Reduction Act SummaryU.S. Senator Tim KaineÎncă nu există evaluări
- Emergency Medicine - Med RevisionsDocument69 paginiEmergency Medicine - Med RevisionsswamysamsonÎncă nu există evaluări
- Emergency Medicine CritiquesDocument9 paginiEmergency Medicine CritiqueskayalÎncă nu există evaluări
- Heroin in ColoradoDocument62 paginiHeroin in ColoradoMichael_Lee_RobertsÎncă nu există evaluări
- 2023-11 - Fentanyl Precursor Submission CDPCDocument12 pagini2023-11 - Fentanyl Precursor Submission CDPCCDPCÎncă nu există evaluări
- Impactoftheopioid Epidemic: Eric J. Lavonas,, Cameron DezfulianDocument17 paginiImpactoftheopioid Epidemic: Eric J. Lavonas,, Cameron DezfulianVlady78Încă nu există evaluări
- 9b) Medical Complications of Drug TakingDocument19 pagini9b) Medical Complications of Drug TakingDr. Zirwa AsimÎncă nu există evaluări
- Practice Questions - EDNDocument6 paginiPractice Questions - EDNKaren BlancoÎncă nu există evaluări
- The Negative Effects of Drugs in SocietyDocument29 paginiThe Negative Effects of Drugs in SocietySantiago FragaÎncă nu există evaluări
- Michigan Opioid Settlement Funds ToolkitDocument29 paginiMichigan Opioid Settlement Funds ToolkitBrandon ChewÎncă nu există evaluări
- ATSP (Asked To See Patient) BookletDocument24 paginiATSP (Asked To See Patient) BookletCindy WongÎncă nu există evaluări
- Product Monograph SuboxoneDocument28 paginiProduct Monograph SuboxoneAÎncă nu există evaluări
- Ohio Opioid Overdose StudyDocument5 paginiOhio Opioid Overdose StudyShannon StowersÎncă nu există evaluări
- SIAC-2021-134 - Utah DMI Fentanyl ReportDocument27 paginiSIAC-2021-134 - Utah DMI Fentanyl ReportJeremy HarrisÎncă nu există evaluări
- Dpa Drug Induced Homicide Report 0Document80 paginiDpa Drug Induced Homicide Report 0Tahsina A MalihaÎncă nu există evaluări
- NIOSH LODD Report On Fatal May 2019 Shooting of Wis. FirefighterDocument30 paginiNIOSH LODD Report On Fatal May 2019 Shooting of Wis. FirefighterepraetorianÎncă nu există evaluări
- Research Paper Final DraftDocument17 paginiResearch Paper Final Draftapi-740628337Încă nu există evaluări
- Heroin Power PointDocument18 paginiHeroin Power Pointapi-280936182Încă nu există evaluări
- International Journal of Pharmacy Practice AbstractsDocument40 paginiInternational Journal of Pharmacy Practice AbstractsFabiola NogaÎncă nu există evaluări
- Strategies") .: Exhibit E List of Opioid Remediation UsesDocument15 paginiStrategies") .: Exhibit E List of Opioid Remediation UsesFergus Burns0% (1)
- Benzie County Draft Opioid Settlement RFPDocument8 paginiBenzie County Draft Opioid Settlement RFPColin MerryÎncă nu există evaluări
- 2015-08-20 St. Mary's County TimesDocument32 pagini2015-08-20 St. Mary's County TimesSouthern Maryland OnlineÎncă nu există evaluări
- Cocaine and HeroinDocument48 paginiCocaine and Heroinzio riaÎncă nu există evaluări
- Intro To HS FinalDocument16 paginiIntro To HS FinalsepehrghfÎncă nu există evaluări
- NaloxBox Press Event Agenda and News ReleaseDocument5 paginiNaloxBox Press Event Agenda and News ReleaseABC6/FOX28Încă nu există evaluări
- Opioid Settlement Fund Advisory Board ReportDocument652 paginiOpioid Settlement Fund Advisory Board ReportCapitol PressroomÎncă nu există evaluări
- Safety Advice NaloxoneDocument3 paginiSafety Advice NaloxoneWDIV/ClickOnDetroitÎncă nu există evaluări