S-ar putea să vă placă și
- InfertilityDocument14 paginiInfertilityDrChauhanÎncă nu există evaluări
- Intern Handbook 2009-2010Document32 paginiIntern Handbook 2009-2010Վարդան ՊապոյանÎncă nu există evaluări
- Pelvic AnatomyDocument106 paginiPelvic AnatomyRosu George100% (1)
- Post MenopauseDocument59 paginiPost Menopausemayuri zanwar100% (1)
- Feeding A Dairy CowDocument31 paginiFeeding A Dairy CowFrancis Onyango OduorÎncă nu există evaluări
- Guide To The Intercollegiate MRCS Examination - Singapore 2012Document55 paginiGuide To The Intercollegiate MRCS Examination - Singapore 2012juweriyÎncă nu există evaluări
- Gross Anatomy of The Pelvis & Perineum DR Ogedengbe O.ODocument162 paginiGross Anatomy of The Pelvis & Perineum DR Ogedengbe O.OKolawole Adesina KehindeÎncă nu există evaluări
- Omohyoid Muscle PDFDocument7 paginiOmohyoid Muscle PDFVarun ArunagiriÎncă nu există evaluări
- Office Gynecology: Princess Cony CayabaDocument60 paginiOffice Gynecology: Princess Cony CayabaCarla Dela CruzÎncă nu există evaluări
- Powerpoint-Menopause DR JoharaDocument26 paginiPowerpoint-Menopause DR JoharaSofia Pranacipta0% (1)
- Stroke - Final ReportDocument16 paginiStroke - Final ReportgolokipokÎncă nu există evaluări
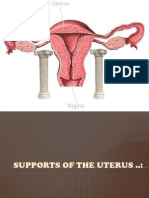
- Supports of The UterusDocument20 paginiSupports of The UterusAshwin Prem Solomon100% (1)
- Blood Supply Pelvic OrgansDocument39 paginiBlood Supply Pelvic OrgansoliviaÎncă nu există evaluări
- Gynecology: by DR - Mohammad Z. Abu Sheikha@Document43 paginiGynecology: by DR - Mohammad Z. Abu Sheikha@صقر حورانÎncă nu există evaluări
- The PelvisDocument44 paginiThe PelvisSadatHamisÎncă nu există evaluări
- Reproductive EndocrinologyDocument18 paginiReproductive EndocrinologyAnonymous hkWIKjoXFVÎncă nu există evaluări
- Anchor Speech On WorkshopDocument6 paginiAnchor Speech On WorkshopPabhat Kumar100% (2)
- Abdominal Ultrasound Anatomy.: DR/ Abd Allah Nazeer. MDDocument50 paginiAbdominal Ultrasound Anatomy.: DR/ Abd Allah Nazeer. MDAri Dwi PrasetyoÎncă nu există evaluări
- Chronic Pelvic Pain2010Document48 paginiChronic Pelvic Pain2010Feruza SultanmuratovaÎncă nu există evaluări
- TOG Vaginal HysterectomyDocument6 paginiTOG Vaginal HysterectomyYasmin AlkhatibÎncă nu există evaluări
- The Male Reproductive SystemDocument14 paginiThe Male Reproductive SystemmarkkkkkkkheeessÎncă nu există evaluări
- Infertility IDocument36 paginiInfertility Idr_asaleh100% (1)
- Surgical Techniques For Prostate Cancer, 1E (2015)Document137 paginiSurgical Techniques For Prostate Cancer, 1E (2015)DiahaÎncă nu există evaluări
- Levator Ani SyndromeDocument24 paginiLevator Ani SyndromeKavya KavyasujathaÎncă nu există evaluări
- Obstetrics and Gynecological InstrumentsDocument31 paginiObstetrics and Gynecological InstrumentsGAYATHRI RAKESHÎncă nu există evaluări
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 paginiDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- Burt and Eklund's Dentistry, Dental Practice, and The Community, 7th EditionDocument330 paginiBurt and Eklund's Dentistry, Dental Practice, and The Community, 7th EditionPhuong Thao75% (4)
- NURS 627 Case Study PaperDocument11 paginiNURS 627 Case Study PaperJaclyn Strangie100% (4)
- Frontal Lobe: Elaborated By: Jeman Nicolae Horaicu Iuliana-Gabriela Group 2124Document7 paginiFrontal Lobe: Elaborated By: Jeman Nicolae Horaicu Iuliana-Gabriela Group 2124Horaicu GabrielaÎncă nu există evaluări
- Magic Roadshow 6Document87 paginiMagic Roadshow 6RickÎncă nu există evaluări
- 3 Most Common Biochemical ImbalancesDocument4 pagini3 Most Common Biochemical Imbalancescarlos100% (1)
- Post Radical Prostatectomy Penile Rehabilitation - AUA Update Series 2008Document8 paginiPost Radical Prostatectomy Penile Rehabilitation - AUA Update Series 2008Kevin ZornÎncă nu există evaluări
- Robotic UrologyDocument279 paginiRobotic UrologyZICOÎncă nu există evaluări
- Female Urology - Urogynecology - and Voiding Dysfunction PDFDocument973 paginiFemale Urology - Urogynecology - and Voiding Dysfunction PDFBelinda TendeananÎncă nu există evaluări
- Anatomy Spotter GI and Repro Answers FinalDocument12 paginiAnatomy Spotter GI and Repro Answers FinalAdiShineÎncă nu există evaluări
- Donna Shoupe: EditorDocument1.112 paginiDonna Shoupe: Editordr Farah Imad AliÎncă nu există evaluări
- Laparoscopic NephrectomyDocument62 paginiLaparoscopic Nephrectomydoc_xia48420% (1)
- Anatomy of The Abdominal Wall - UpToDate2019 PDFDocument21 paginiAnatomy of The Abdominal Wall - UpToDate2019 PDFGerii Pucllas VillarÎncă nu există evaluări
- Surgical Female Urogenital Anatomy - UpToDateDocument57 paginiSurgical Female Urogenital Anatomy - UpToDateErickÎncă nu există evaluări
- Vesicovaginal FistulaDocument7 paginiVesicovaginal Fistuladrnareshkumar3281Încă nu există evaluări
- Images of Circumcision Complications Adult Circumcision Images Complications of Circumcision - Your Whole BabyDocument1 paginăImages of Circumcision Complications Adult Circumcision Images Complications of Circumcision - Your Whole BabyPhoenixxx BeyÎncă nu există evaluări
- Multiple Atrophy System (MSA) Trust Caregiver's GuideDocument11 paginiMultiple Atrophy System (MSA) Trust Caregiver's GuideThe Multiple System Atrophy CoalitionÎncă nu există evaluări
- UROLOGYDocument222 paginiUROLOGYBeso DavitashviliÎncă nu există evaluări
- Non-Surgical and Surgical Management of Pelvic OrgDocument10 paginiNon-Surgical and Surgical Management of Pelvic OrgAhmed AnwarÎncă nu există evaluări
- About Monkey PoxDocument3 paginiAbout Monkey PoxObakoma Josiah100% (1)
- Antireflux Surgery Lich-GregoirDocument16 paginiAntireflux Surgery Lich-GregoircristiangelsÎncă nu există evaluări
- Clinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumDocument20 paginiClinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumJacobMsangÎncă nu există evaluări
- Paediatric UrologyDocument194 paginiPaediatric UrologyTrishenth FonsekaÎncă nu există evaluări
- Sacrococcygeal Teratoma (SCT)Document5 paginiSacrococcygeal Teratoma (SCT)IOSRjournalÎncă nu există evaluări
- Total Pelvic ExenterationDocument13 paginiTotal Pelvic ExenterationRirin Wahyuni100% (1)
- Genital ProlapseDocument13 paginiGenital ProlapsesmbawasainiÎncă nu există evaluări
- Pediatric UrologyDocument80 paginiPediatric UrologySav GaÎncă nu există evaluări
- WP GynaeExams4Document37 paginiWP GynaeExams4Ahsan JamÎncă nu există evaluări
- The Gynecologic History and Pelvic Examination Up To Date 2016Document14 paginiThe Gynecologic History and Pelvic Examination Up To Date 2016Mateo GlÎncă nu există evaluări
- Handout and Questions of HysterosalpingDocument12 paginiHandout and Questions of Hysterosalpingahmad shaltout100% (2)
- Clinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaDocument17 paginiClinical Practice Guideline For The Management of Anorectal Abscess Fistula-In-Ano and Rectovaginal FistulaAlivia HanumÎncă nu există evaluări
- Transfemoral Above Knee AmputationDocument4 paginiTransfemoral Above Knee AmputationMarthaLhtÎncă nu există evaluări
- Role of Pathya Apathya in VranaDocument6 paginiRole of Pathya Apathya in VranaEditor IJTSRDÎncă nu există evaluări
- KEMH Guidelines On Cardiac Disease in PregnancyDocument7 paginiKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaÎncă nu există evaluări
- Narrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowDocument12 paginiNarrative Review of Pelvic Floor Muscle Training For Childbearing Women-Why, When, What, and HowLéa Cinthia Silva do NascimentoÎncă nu există evaluări
- Genitalexam Ingirls PDFDocument12 paginiGenitalexam Ingirls PDFjprakashjjÎncă nu există evaluări
- Obstetric Gynaecology Jan 11Document32 paginiObstetric Gynaecology Jan 11selvie87Încă nu există evaluări
- 26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFDocument57 pagini26.7.16-Approach To Ambiguous Genitalia - Is It A Boy or Girl PDFBlueash BehÎncă nu există evaluări
- Pop QDocument45 paginiPop QObgyn Maret2016Încă nu există evaluări
- Congenital Malformations of The Female Genital TractDocument7 paginiCongenital Malformations of The Female Genital TractDo le QuangÎncă nu există evaluări
- 2008, Vol.92, Issues 5, Women's HealthDocument312 pagini2008, Vol.92, Issues 5, Women's HealthHussain OudahÎncă nu există evaluări
- Gynecology and ObstetricsDocument190 paginiGynecology and Obstetricsbhesh_seanÎncă nu există evaluări
- Urinary Tract Infection Diet: A Beginner’s 4-Step Guide for Women on Managing UTI Through Diet, With Sample Curated RecipesDe la EverandUrinary Tract Infection Diet: A Beginner’s 4-Step Guide for Women on Managing UTI Through Diet, With Sample Curated RecipesÎncă nu există evaluări
- Apothio Hemp LawsuitDocument58 paginiApothio Hemp LawsuitLaw&CrimeÎncă nu există evaluări
- Role of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicDocument7 paginiRole of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicJHÎncă nu există evaluări
- 2019 - Postoperative Healing Assessment Using Cannabinoids in Oral SurgeryDocument7 pagini2019 - Postoperative Healing Assessment Using Cannabinoids in Oral SurgerycorcarolÎncă nu există evaluări
- AP Bio Lab 3Document18 paginiAP Bio Lab 3zzmasterÎncă nu există evaluări
- DR Antonious CV N & AEDocument27 paginiDR Antonious CV N & AEdoctorantoniÎncă nu există evaluări
- P.E EssayDocument2 paginiP.E EssayMia LucinaÎncă nu există evaluări
- Fibroadenoma Mammae of The BreastDocument15 paginiFibroadenoma Mammae of The Breastirvanie100% (1)
- Hydrogen Sulfide FactDocument2 paginiHydrogen Sulfide FactAgriSafeÎncă nu există evaluări
- Dalay Panishment of FormalinDocument4 paginiDalay Panishment of Formalinmutiara defiskaÎncă nu există evaluări
- Paket B Soal Listening TO US MGMP B.Inggris DKI 2023Document14 paginiPaket B Soal Listening TO US MGMP B.Inggris DKI 2023X MIPA-E /10 Garnis Trie AdistyÎncă nu există evaluări
- Management Guide Commercial Cage English Vs L0260-6Document88 paginiManagement Guide Commercial Cage English Vs L0260-6Juliana de Souza Granja BarrosÎncă nu există evaluări
- Does The Behaviour of Using Electronic Cigarette Correlates With Respiratory Disease Symptoms?Document6 paginiDoes The Behaviour of Using Electronic Cigarette Correlates With Respiratory Disease Symptoms?Ninuk KurniawatiÎncă nu există evaluări
- Mandibular NerveDocument3 paginiMandibular Nervervinluan.dentÎncă nu există evaluări
- Active Transport by ATP-Powered Pumps - Molecular Cell Biology - NCBI BookshelfDocument10 paginiActive Transport by ATP-Powered Pumps - Molecular Cell Biology - NCBI BookshelfMuhammad KhanÎncă nu există evaluări
- Endocrine Physiology - Part 3 Parathyroid GlandDocument30 paginiEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraÎncă nu există evaluări
- 11 Biology Notes ch02 Biological ClassificationDocument8 pagini11 Biology Notes ch02 Biological ClassificationDivyaa SreekumarÎncă nu există evaluări
- Endometriosis: Endometriosis: Symptoms, Treatment, DiagnosisDocument4 paginiEndometriosis: Endometriosis: Symptoms, Treatment, DiagnosisrizkiaautikasariÎncă nu există evaluări
- Pasteur Eng MiddleDocument4 paginiPasteur Eng MiddleRoykoÎncă nu există evaluări
- Medical Certificate: C.S. FORM No. 41Document1 paginăMedical Certificate: C.S. FORM No. 41adoriza0218Încă nu există evaluări
- Cells - 1 V2 (Euks, Proks & Viruses)Document9 paginiCells - 1 V2 (Euks, Proks & Viruses)mormerodÎncă nu există evaluări
- 2016 AEIS Instructions To Candidates PDFDocument4 pagini2016 AEIS Instructions To Candidates PDFThomasÎncă nu există evaluări