S-ar putea să vă placă și
- Cardiovascular DrugsDocument6 paginiCardiovascular Drugslhayes123488% (16)
- Assessment Info NotesDocument3 paginiAssessment Info NotesDiana DeckerÎncă nu există evaluări
- Pharmacology of HypertensionDocument4 paginiPharmacology of HypertensionFlower100% (1)
- Insulin Comparison ChartDocument1 paginăInsulin Comparison Chartmaend87Încă nu există evaluări
- Family Names of DrugsDocument1 paginăFamily Names of DrugsangelÎncă nu există evaluări
- Remembering Medication ClassificationsDocument2 paginiRemembering Medication ClassificationsGVHHÎncă nu există evaluări
- Pharmacology-ATI 150 Drug Cards PDFDocument4 paginiPharmacology-ATI 150 Drug Cards PDFhollyÎncă nu există evaluări
- Know Common Disease ManagementDocument14 paginiKnow Common Disease Managementcdx25Încă nu există evaluări
- Guide To Diabetes MedicationsDocument2 paginiGuide To Diabetes MedicationsJianhua ShiÎncă nu există evaluări
- Summary of Antidiabetic Drugs PDFDocument3 paginiSummary of Antidiabetic Drugs PDFZinc YuloÎncă nu există evaluări
- Hypertension Drugs Cheat Sheet: by ViaDocument3 paginiHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharÎncă nu există evaluări
- Renal Guide and Charts: AlbuminDocument16 paginiRenal Guide and Charts: AlbuminYaima JimenezÎncă nu există evaluări
- Pharmacology Important Things To RememberDocument5 paginiPharmacology Important Things To RememberHydie100% (1)
- Classification of Drugs PDFDocument15 paginiClassification of Drugs PDFmuhammad ihtisham ul hassanÎncă nu există evaluări
- Labs Electrolyte ChartDocument1 paginăLabs Electrolyte ChartmdcmepÎncă nu există evaluări
- Heart Failure Topic DiscussionDocument11 paginiHeart Failure Topic Discussionapi-665372449Încă nu există evaluări
- @ Shopwithkey On Etsy Perfusion Drug Classification ChartDocument8 pagini@ Shopwithkey On Etsy Perfusion Drug Classification ChartSutanyaÎncă nu există evaluări
- DrugsDocument155 paginiDrugsAkankshaÎncă nu există evaluări
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 paginiPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SÎncă nu există evaluări
- With Dr. Susan Lipsett: Community Acquired PneumoniaDocument1 paginăWith Dr. Susan Lipsett: Community Acquired PneumoniaJayantiÎncă nu există evaluări
- ACE InhibitorsDocument8 paginiACE InhibitorsJohn HillÎncă nu există evaluări
- Neuro Psych - Antiepileptic Drug ChartDocument5 paginiNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocument43 paginiNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- Kaplan Notes. ExamenSO IMPORTANTDocument145 paginiKaplan Notes. ExamenSO IMPORTANTLisaÎncă nu există evaluări
- Pharmocology Drug Cards: InnovarDocument33 paginiPharmocology Drug Cards: InnovarfaizaÎncă nu există evaluări
- Oman Prometric Exam NotesDocument417 paginiOman Prometric Exam NotesMuhammad Amin93% (14)
- PEDIA - TachypneaDocument12 paginiPEDIA - TachypneaAlvin Germo PasuquinÎncă nu există evaluări
- Common Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesDocument2 paginiCommon Drug Stems Cheat Sheet: Drug Stem Drug Class And/or Stem Explanation ExamplesjthsÎncă nu există evaluări
- Mu 002Document10 paginiMu 002chandanÎncă nu există evaluări
- Prefix Suffix MnemonicsDocument5 paginiPrefix Suffix MnemonicsPj MontecilloÎncă nu există evaluări
- ACE InhibitorsDocument26 paginiACE Inhibitorsali mohammedÎncă nu există evaluări
- Mechanism of Action For Each Class of AntiDocument146 paginiMechanism of Action For Each Class of AntiReynaldo RiveraÎncă nu există evaluări
- Drug CardsDocument3 paginiDrug CardsDave HillÎncă nu există evaluări
- Drugclasses Pharmacologypart 1 PDFDocument25 paginiDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- HESI Qbank From QuizletDocument11 paginiHESI Qbank From Quizletnana100% (4)
- Chronic Kidney Disease Case StudyDocument96 paginiChronic Kidney Disease Case StudyJUDE ARIZALAÎncă nu există evaluări
- Drug Interactions: What Is An Interaction?Document4 paginiDrug Interactions: What Is An Interaction?Leyla MajundaÎncă nu există evaluări
- Drugs To Watch With WARFARINDocument3 paginiDrugs To Watch With WARFARINRajendra RaiÎncă nu există evaluări
- 300 QuestionsDocument34 pagini300 QuestionsAhmed Assem78% (9)
- 7 Drug StudyDocument17 pagini7 Drug StudyMa. Mechile MartinezÎncă nu există evaluări
- AnxietyDocument5 paginiAnxietyJohn HolmesÎncă nu există evaluări
- Beta BlockersDocument1 paginăBeta BlockersShrikant ThakurÎncă nu există evaluări
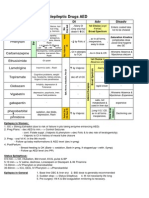
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 paginăAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Încă nu există evaluări
- Pharmacology FirecrackerDocument37 paginiPharmacology FirecrackerRehan Usman100% (1)
- Anticoagulants Drug TableDocument1 paginăAnticoagulants Drug TableNicole HoÎncă nu există evaluări
- Grapefruit Juice and Drug Interactions - 0717Document2 paginiGrapefruit Juice and Drug Interactions - 0717Asri YaniÎncă nu există evaluări
- Ace Inhibitors MnemonicDocument1 paginăAce Inhibitors MnemonicGirish Waru0% (2)
- Agents Causing Coma or SeizuresDocument3 paginiAgents Causing Coma or SeizuresShaira Aquino VerzosaÎncă nu există evaluări
- Argus 5 1 Test CasesDocument11 paginiArgus 5 1 Test CasespponnapatiÎncă nu există evaluări
- Anti HypertensivesDocument15 paginiAnti HypertensivesFaye MillanesÎncă nu există evaluări
- Vancomycin Protocol RQHRDocument15 paginiVancomycin Protocol RQHRl1o2stÎncă nu există evaluări
- Pharmacology Drug ChartDocument50 paginiPharmacology Drug ChartEssentialForLivingÎncă nu există evaluări
- Insulin Chart 05032012 PDFDocument1 paginăInsulin Chart 05032012 PDFTiffany CrittendenÎncă nu există evaluări
- IV PO Conversion CAPDocument3 paginiIV PO Conversion CAPdamondouglasÎncă nu există evaluări
- Pharm Expansion 17 NDFDocument1 paginăPharm Expansion 17 NDFNokz M. Raki-inÎncă nu există evaluări
- Assessing Abdominal Distensión After GastrectomyDocument1 paginăAssessing Abdominal Distensión After GastrectomyEunice CortésÎncă nu există evaluări
- Template Drug Card1Document1 paginăTemplate Drug Card1Kay TaylorÎncă nu există evaluări
- Pharmacology Notes (Chapter 20 and 21)Document2 paginiPharmacology Notes (Chapter 20 and 21)graycorypÎncă nu există evaluări
- Antibiotic GuideDocument6 paginiAntibiotic GuideAnnTran100% (1)
- ATI Med Template Vitamin DDocument1 paginăATI Med Template Vitamin DHeather MoralesÎncă nu există evaluări
- Common Medications UsedDocument3 paginiCommon Medications UsedRay Michael CasupananÎncă nu există evaluări
- NORADRENALINE (Norepinephrine) : Presentation DescriptionDocument3 paginiNORADRENALINE (Norepinephrine) : Presentation DescriptionMutiaraÎncă nu există evaluări
- Generic Name FurosemideDocument1 paginăGeneric Name FurosemideChristopher LeeÎncă nu există evaluări
- Pharm Drug Outline AdrDocument1 paginăPharm Drug Outline AdrCess Lagera YbanezÎncă nu există evaluări
- Agents For Anemia, Hematopoietic, & Myeloproliferative DiseasesDocument2 paginiAgents For Anemia, Hematopoietic, & Myeloproliferative Diseaseskaylakmills_10135868Încă nu există evaluări
- 14 Fun Facts About Your Heart: Educational VersionDe la Everand14 Fun Facts About Your Heart: Educational VersionÎncă nu există evaluări
- NURSING CARE OF ADULTS II: Passbooks Study GuideDe la EverandNURSING CARE OF ADULTS II: Passbooks Study GuideÎncă nu există evaluări
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Platinum Formulary 2016Document61 paginiPlatinum Formulary 2016jÎncă nu există evaluări
- Hypertension PDFDocument6 paginiHypertension PDFRaouf Ra'fat SolimanÎncă nu există evaluări
- Preparation of Extemporaneous Oral Liquid in The Hospital PharmacyDocument15 paginiPreparation of Extemporaneous Oral Liquid in The Hospital PharmacyAhmed YousefÎncă nu există evaluări
- DRUG StudyDocument43 paginiDRUG StudyNathalie Faith CotengÎncă nu există evaluări
- DIURETICSDocument40 paginiDIURETICSNiña Jean Tormis AldabaÎncă nu există evaluări
- GPAT Handy NotesDocument38 paginiGPAT Handy NotescuambyahooÎncă nu există evaluări
- Pharmacology ReviewerDocument28 paginiPharmacology ReviewerYuki Xairah TunayÎncă nu există evaluări
- Template ArticleDocument14 paginiTemplate ArticleLisda Amalia P. 17.010Încă nu există evaluări
- Pharma Cardio Respi and Repro NclexdocxDocument8 paginiPharma Cardio Respi and Repro NclexdocxJhayneÎncă nu există evaluări
- Antihypertensive AgentDocument2 paginiAntihypertensive AgentMuhammad Naufal FadhillahÎncă nu există evaluări
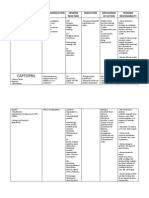
- CaptoprilDocument3 paginiCaptoprilapi-3797941100% (1)
- أدوية الضغطDocument2 paginiأدوية الضغطSamalout Specialized HospitalÎncă nu există evaluări
- Drug ListDocument24 paginiDrug Listcicima1016Încă nu există evaluări
- Management Scorpion Sting Journal PDFDocument9 paginiManagement Scorpion Sting Journal PDFDody Tri GusnawanÎncă nu există evaluări
- Pharmacology ReviewerDocument21 paginiPharmacology ReviewerCzairalene QuinzonÎncă nu există evaluări
- Pharmacology Made EasyDocument43 paginiPharmacology Made EasyGauthaman KarunakaranÎncă nu există evaluări
- Banco de Preguntas Cardio SincDocument37 paginiBanco de Preguntas Cardio SincnoahÎncă nu există evaluări
- Drug StudyDocument8 paginiDrug StudyJohn Ronald P. RamosÎncă nu există evaluări
- A Brief History of PharmacologyDocument6 paginiA Brief History of PharmacologyymonnÎncă nu există evaluări
- Guidelines For Avoiding Food-Drug InteractionsDocument5 paginiGuidelines For Avoiding Food-Drug InteractionslnornelasÎncă nu există evaluări
- Amlodipine Captopril MetronidazoleDocument5 paginiAmlodipine Captopril Metronidazolekhrysty1506Încă nu există evaluări