S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Diff Betwn Inlay and Amalgam CavityDocument7 paginiDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Criteria of SelectionDocument12 paginiCriteria of SelectionVinisha Vipin SharmaÎncă nu există evaluări
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocument159 paginiMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaÎncă nu există evaluări
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 paginiNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaÎncă nu există evaluări
- Acupuncture in Dentistry PDFDocument73 paginiAcupuncture in Dentistry PDFVinisha Vipin SharmaÎncă nu există evaluări
- Challenges in Working Length DeterminationDocument101 paginiChallenges in Working Length DeterminationVinisha Vipin SharmaÎncă nu există evaluări
- Eaat 14 I 1 P 217Document6 paginiEaat 14 I 1 P 217Vinisha Vipin SharmaÎncă nu există evaluări
- Content ServerDocument5 paginiContent ServerVinisha Vipin SharmaÎncă nu există evaluări
- Glide Path PreparationDocument5 paginiGlide Path PreparationVinisha Vipin SharmaÎncă nu există evaluări
- Show TextDocument1 paginăShow TextVinisha Vipin SharmaÎncă nu există evaluări
- PRISMA-P Statement - Moher Sys Rev Jan 2015Document9 paginiPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaÎncă nu există evaluări
- Some Basics of LasersDocument102 paginiSome Basics of LasersVinisha Vipin SharmaÎncă nu există evaluări
- Laser in Conservative Dentistry & EndodonticsDocument75 paginiLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaÎncă nu există evaluări
- Dentin HypersensitivityDocument62 paginiDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Content ServerDocument6 paginiContent ServerVinisha Vipin SharmaÎncă nu există evaluări
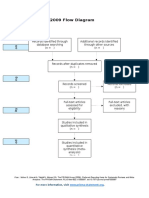
- PRISMA 2009 Flow Diagram: For More Information, VisitDocument1 paginăPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaÎncă nu există evaluări
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocument5 paginiPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaÎncă nu există evaluări
- EchsDocument20 paginiEchsVinisha Vipin SharmaÎncă nu există evaluări
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocument5 paginiCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaÎncă nu există evaluări
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocument5 paginiNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaÎncă nu există evaluări
- Esthetic Alternatives To AmalgamDocument15 paginiEsthetic Alternatives To AmalgamVinisha Vipin SharmaÎncă nu există evaluări
- Pin Retained RestorationDocument31 paginiPin Retained RestorationVinisha Vipin SharmaÎncă nu există evaluări
- Clarks Cavity PreparationDocument10 paginiClarks Cavity PreparationVinisha Vipin SharmaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- TRM34 Preparation of Calculations Rev5Document5 paginiTRM34 Preparation of Calculations Rev5TuanÎncă nu există evaluări
- Krunker ModMenuDocument10 paginiKrunker ModMenuCody Kartavya0% (1)
- Nachi Special SteelsDocument20 paginiNachi Special SteelsBambang MulyantoÎncă nu există evaluări
- BX 3010 (0C)Document362 paginiBX 3010 (0C)Lâm Hồ Ngọc HãnÎncă nu există evaluări
- Large Volume PoursDocument7 paginiLarge Volume PoursgordonÎncă nu există evaluări
- Company Profile Traya Lintas PersadaDocument24 paginiCompany Profile Traya Lintas PersadaAyu Catra KastaraÎncă nu există evaluări
- Experiment 1Document5 paginiExperiment 1Cheng BauzonÎncă nu există evaluări
- Hoses & AppliancesDocument92 paginiHoses & Appliancestheguy 21100% (1)
- Gogostemcells StudentpagesDocument2 paginiGogostemcells Studentpagesapi-356824125Încă nu există evaluări
- 1 5 1Document5 pagini1 5 1daemsalÎncă nu există evaluări
- Top Gun I-ARC 130Document9 paginiTop Gun I-ARC 130Tom PleysierÎncă nu există evaluări
- Lab Manual - DEDocument41 paginiLab Manual - DEAnkur Giri100% (2)
- SLM 1 CARPENTRY 10 Revalidated and Language 1st QuarterDocument8 paginiSLM 1 CARPENTRY 10 Revalidated and Language 1st Quarterash hshsÎncă nu există evaluări
- SRI FireFighting Equipments 2012 PDFDocument46 paginiSRI FireFighting Equipments 2012 PDFsullamsÎncă nu există evaluări
- KinematicsDocument33 paginiKinematicsErik MagnoÎncă nu există evaluări
- KNS2163 Week1Document32 paginiKNS2163 Week1Nurul QurratuÎncă nu există evaluări
- Assessment of Rotational Capacity Test Procedure FINALDocument21 paginiAssessment of Rotational Capacity Test Procedure FINALzaheerahmed77Încă nu există evaluări
- Instalación Zapata Case 9010Document5 paginiInstalación Zapata Case 9010Miguel Angel Herrera MartinezÎncă nu există evaluări
- Foreword by Brett Queener - Agile Product Management With Scrum - Creating Products That Customers LoveDocument3 paginiForeword by Brett Queener - Agile Product Management With Scrum - Creating Products That Customers LoveJoao Paulo MouraÎncă nu există evaluări
- Johnloomis Org Ece563 Notes Geom Resize ImresizeDocument10 paginiJohnloomis Org Ece563 Notes Geom Resize ImresizeAdrian Jose Costa OspinoÎncă nu există evaluări
- BITS Herald Summer Issue 2013Document23 paginiBITS Herald Summer Issue 2013Bits Herald100% (1)
- Design of Well FoundationDocument31 paginiDesign of Well FoundationAshish Karki97% (32)
- Ford's PHEV Fact SheetDocument1 paginăFord's PHEV Fact SheetFord Motor Company100% (2)
- Alien Legacy-Manual PDFDocument93 paginiAlien Legacy-Manual PDFMark BallingerÎncă nu există evaluări
- Deception & Detection-On Amazon Reviews DatasetDocument9 paginiDeception & Detection-On Amazon Reviews Datasetyavar khanÎncă nu există evaluări
- 023 POL902.00 CB1Q3934en 01 ModBusDocument4 pagini023 POL902.00 CB1Q3934en 01 ModBusEvandroRodriguesÎncă nu există evaluări
- Toshiba Satellite L650 12Q Laptop ManualDocument229 paginiToshiba Satellite L650 12Q Laptop ManualTasos KachpanisÎncă nu există evaluări
- Cathodic Protection System Inspection and Test PlanDocument10 paginiCathodic Protection System Inspection and Test PlanNoor A QasimÎncă nu există evaluări
- Math 1030 Working in The YardDocument4 paginiMath 1030 Working in The Yardapi-313345556Încă nu există evaluări
- Sub Test Mole Concept PDFDocument7 paginiSub Test Mole Concept PDFVIKAS GARGÎncă nu există evaluări