S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Closing Ranks & Allotment Round 2 - NEET SS 2018 PDFDocument79 paginiClosing Ranks & Allotment Round 2 - NEET SS 2018 PDFlakshminivas PingaliÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Tattoos Body PiercingsDocument17 paginiTattoos Body PiercingsSaad MotawéaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- 2015 Movement DisordersDocument567 pagini2015 Movement DisordersAndreea Raluca CimpoiÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Water LaceDocument67 paginiWater LaceRekha BipinÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Fortis Hospitals - Marathah.Document4 paginiFortis Hospitals - Marathah.anuperickujurÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Postural, DrainageDocument7 paginiPostural, DrainageJames ThompsonÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- 05 Lifting and Moving PatientsDocument48 pagini05 Lifting and Moving PatientsYunita Evi Indrani100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Panoramic Radiography 11Document47 paginiPanoramic Radiography 11empormeniÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Patient Health ProfileDocument4 paginiPatient Health ProfileChristopher WuÎncă nu există evaluări
- Efficient Antibiotic Bead Production TechniqueDocument5 paginiEfficient Antibiotic Bead Production Techniqueratnav_ratanÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Eric Thorhauer CVDocument7 paginiEric Thorhauer CVapi-251923314Încă nu există evaluări
- Aesculap Basic Sets of Neurosurgical Instruments PDFDocument10 paginiAesculap Basic Sets of Neurosurgical Instruments PDFyudiÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- LIFE Kite Flying Sponsorship LetterDocument3 paginiLIFE Kite Flying Sponsorship LetterMarjorie CuaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Anatomy of The KidneyDocument13 paginiAnatomy of The KidneyChristi NaldoÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Moondance Midwifery, Preparing For A Home BirthDocument5 paginiMoondance Midwifery, Preparing For A Home BirthlimestonebutterflyÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 2021 - July - INI-CET - Open Round Seat Allocation - 3.8 - Final Vacant Seats For Open RoundDocument5 pagini2021 - July - INI-CET - Open Round Seat Allocation - 3.8 - Final Vacant Seats For Open RoundAnjali GuptaÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Classification Proposed by Seddon in 1943 Was Generally Accepted But Rarely UsedDocument7 paginiClassification Proposed by Seddon in 1943 Was Generally Accepted But Rarely UsedMd Ahsanuzzaman PinkuÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Ross ScoreDocument7 paginiRoss Scoreradwika antyÎncă nu există evaluări
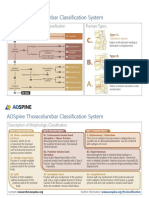
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 paginiAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- MMDSTDocument2 paginiMMDSTBianca MolinaÎncă nu există evaluări
- Access CavityDocument35 paginiAccess CavitySaca AnastasiaÎncă nu există evaluări
- Health: Living in EnglishDocument8 paginiHealth: Living in EnglishPaula CalvoÎncă nu există evaluări
- Plan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Document7 paginiPlan of The Course Anatomy and Clinical Anatomy: Academic Year 2013/2014Rinor MujajÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- MG II S2-Hospital-2Document5 paginiMG II S2-Hospital-2Iuliana RaduÎncă nu există evaluări
- Pathophysiology of Variceal Bleeding in CirrhoticsDocument8 paginiPathophysiology of Variceal Bleeding in Cirrhoticsanon_914506742Încă nu există evaluări
- GingivectomyDocument51 paginiGingivectomyWendy JengÎncă nu există evaluări
- PQCNC ASNS Learning Session - Integrating The Sepsis Calculator Into The EMRDocument35 paginiPQCNC ASNS Learning Session - Integrating The Sepsis Calculator Into The EMRkcochranÎncă nu există evaluări
- Cerebral PalsyDocument4 paginiCerebral Palsyapi-165286810Încă nu există evaluări
- American Heart Association: Brave Little Hearts SADocument10 paginiAmerican Heart Association: Brave Little Hearts SAAnonymous SeQpeTÎncă nu există evaluări
- Chapter 8, Part B - The Spinal Cord!Document9 paginiChapter 8, Part B - The Spinal Cord!Putamen NongchaiÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)