S-ar putea să vă placă și
- NICU Survival GuideDocument14 paginiNICU Survival Guidesedaka26Încă nu există evaluări
- Amniiotic Band Syndrome Cleft Lip/palate Congenital Limb Defects Duodenal AtresiaDocument18 paginiAmniiotic Band Syndrome Cleft Lip/palate Congenital Limb Defects Duodenal AtresiaMJ Amarillo100% (3)
- NICU Pocket GuideDocument28 paginiNICU Pocket GuideCharles S. Williams RRT, AE-C86% (7)
- NICU BrainDocument9 paginiNICU BrainSarah Boyce Cernik100% (1)
- Patient Worksheet - NICU 2-PatientDocument2 paginiPatient Worksheet - NICU 2-PatientJerry G75% (4)
- Neonatal EmergenciesDocument123 paginiNeonatal EmergenciesMaria Babette Almazan Talavera100% (2)
- Neonatal Resuscitation Program: 7 EditionDocument64 paginiNeonatal Resuscitation Program: 7 EditionStacy LuceroÎncă nu există evaluări
- Neonatology Guide for Maternal and Newborn CareDocument8 paginiNeonatology Guide for Maternal and Newborn Caremymamym100% (1)
- Neonatal Reurscitation PDFDocument347 paginiNeonatal Reurscitation PDFAlina Andreica100% (1)
- Nicu Must KnowsDocument7 paginiNicu Must KnowsCyfern100% (2)
- Mechanical Ventilation in NeonatesDocument60 paginiMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- Neonatal Ventilator Vent Set-Up CheatsheetDocument1 paginăNeonatal Ventilator Vent Set-Up CheatsheetRick Frea50% (2)
- NICU ProtocolDocument75 paginiNICU ProtocolCatherine Lee100% (6)
- Manual de RCP - NEONATAL - 7°ED PDFDocument328 paginiManual de RCP - NEONATAL - 7°ED PDFNatanael Librado97% (29)
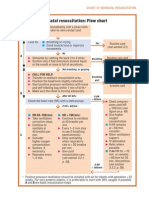
- Neonatal Resuscitation Program Flow ChartDocument3 paginiNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- A Guide To The Newborn Intensive Care Unit (NICU)Document36 paginiA Guide To The Newborn Intensive Care Unit (NICU)Jean Wallace100% (3)
- Neonatal Care Pocket Guide For Hospital Physicians PDFDocument319 paginiNeonatal Care Pocket Guide For Hospital Physicians PDFelmaadawy2002100% (7)
- Stable 2Document115 paginiStable 2Avyel KramÎncă nu există evaluări
- Admission To NICU CA4068v3Document12 paginiAdmission To NICU CA4068v3Hana ChristyantiÎncă nu există evaluări
- Neonatal NotesDocument34 paginiNeonatal Notesgridchan100% (2)
- Neonatal ResucitationDocument47 paginiNeonatal ResucitationLeighton Ricardo WynterÎncă nu există evaluări
- Essential Newborn Resuscitation StepsDocument27 paginiEssential Newborn Resuscitation StepsAnusha Verghese100% (1)
- 66 Neonatal Resuscitation Show Notes 1Document3 pagini66 Neonatal Resuscitation Show Notes 1Rabbani IcksanÎncă nu există evaluări
- NICU Manual Cheat SheetDocument2 paginiNICU Manual Cheat Sheetlori_quintal92% (13)
- AIIMS neonatal seizure protocol highlights causes, types, assessmentDocument18 paginiAIIMS neonatal seizure protocol highlights causes, types, assessmentgitphillipÎncă nu există evaluări
- NICU Orientation ManualDocument27 paginiNICU Orientation Manualsedaka26100% (1)
- NEONATAL INTENSIVE CARE NURSING: Passbooks Study GuideDe la EverandNEONATAL INTENSIVE CARE NURSING: Passbooks Study GuideÎncă nu există evaluări
- Complete Issue NeoReviewsDocument68 paginiComplete Issue NeoReviewsArvin E. PamatianÎncă nu există evaluări
- Newborn Care Hnadbook by 2019 ClassDocument267 paginiNewborn Care Hnadbook by 2019 Classknowledge chanall chanallÎncă nu există evaluări
- NICU Dose Card05Document2 paginiNICU Dose Card05Mohamed Abo SeifÎncă nu există evaluări
- Nicu Survival Guide For ResidentsDocument26 paginiNicu Survival Guide For ResidentspeppepagÎncă nu există evaluări
- DR Johnson On Neonatal Resuscitation Guidelines 041707Document44 paginiDR Johnson On Neonatal Resuscitation Guidelines 041707sameerarswÎncă nu există evaluări
- Interpretting Neonatal Xrays (Click Enable Macros)Document304 paginiInterpretting Neonatal Xrays (Click Enable Macros)John Phamnguyen100% (5)
- Textbook of Neonatal Resuscitation 8th EditionDocument333 paginiTextbook of Neonatal Resuscitation 8th Editionmirandad784100% (1)
- Neonatal Resuscitation ProgramDocument6 paginiNeonatal Resuscitation ProgramRick Frea100% (5)
- NEONATAL RESUSCITATION PROGRAM DiagramDocument1 paginăNEONATAL RESUSCITATION PROGRAM DiagramShanon Mae Pereza LagranaÎncă nu există evaluări
- Neonatal VentilationDocument65 paginiNeonatal VentilationBadr Chaban100% (5)
- Nicu Sheet Date: / / By: Sherif ElgamilyDocument1 paginăNicu Sheet Date: / / By: Sherif ElgamilysherifÎncă nu există evaluări
- Pediatric GI ComplaintsDocument41 paginiPediatric GI ComplaintsGladys SudiyantoÎncă nu există evaluări
- 2011 Pediatric HandbookDocument146 pagini2011 Pediatric Handbooksedaka2680% (5)
- Neonatal Resuscitation: BY DR Babatunde O.TDocument20 paginiNeonatal Resuscitation: BY DR Babatunde O.Tijojo elizabethÎncă nu există evaluări
- NRP Baby Saver III June 2011Document24 paginiNRP Baby Saver III June 2011nursesedÎncă nu există evaluări
- Clinical Nursing Research: Noise Intervention Minimizing Preterm Infants' Exposure To NICU Light andDocument23 paginiClinical Nursing Research: Noise Intervention Minimizing Preterm Infants' Exposure To NICU Light andCleoanne GallegosÎncă nu există evaluări
- Picu PocketbookDocument7 paginiPicu Pocketbookandrahlyn100% (1)
- Pocketbook WHO PediatricsDocument398 paginiPocketbook WHO PediatricsNashria RusdhyÎncă nu există evaluări
- Neonatal Intensive Care Unit (Nicu)Document30 paginiNeonatal Intensive Care Unit (Nicu)Uday Kumar100% (15)
- Quick Hits for Pediatric Emergency MedicineDe la EverandQuick Hits for Pediatric Emergency MedicineCristina M. Zeretzke-BienÎncă nu există evaluări
- Nursing the NeonateDe la EverandNursing the NeonateMaggie MeeksÎncă nu există evaluări
- NEONATAL NURSE PRACTITIONER: Passbooks Study GuideDe la EverandNEONATAL NURSE PRACTITIONER: Passbooks Study GuideÎncă nu există evaluări
- Neonatal Nurse Practitioner A Complete Guide - 2020 EditionDe la EverandNeonatal Nurse Practitioner A Complete Guide - 2020 EditionÎncă nu există evaluări
- Certified Pediatric Emergency Nurse Review: Putting It All TogetherDe la EverandCertified Pediatric Emergency Nurse Review: Putting It All TogetherÎncă nu există evaluări
- Pediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)De la EverandPediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)Încă nu există evaluări
- Neonatal Clinical Pharmacology and TherapeuticsDe la EverandNeonatal Clinical Pharmacology and TherapeuticsEvaluare: 5 din 5 stele5/5 (1)
- Neonatal Nursing: Scope and Standards of PracticeDe la EverandNeonatal Nursing: Scope and Standards of PracticeEvaluare: 4 din 5 stele4/5 (1)
- Intensive Parenting: Surviving the Emotional Journey through the NICUDe la EverandIntensive Parenting: Surviving the Emotional Journey through the NICUÎncă nu există evaluări
- LOW RISK NEONATAL NURSING: Passbooks Study GuideDe la EverandLOW RISK NEONATAL NURSING: Passbooks Study GuideÎncă nu există evaluări
- Inpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)De la EverandInpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)Încă nu există evaluări
- Pediatric Cardiology and Pulmonology: A Practically Painless ReviewDe la EverandPediatric Cardiology and Pulmonology: A Practically Painless ReviewÎncă nu există evaluări
- American Diabetes Association (ADA) gUIDELINESDocument43 paginiAmerican Diabetes Association (ADA) gUIDELINESSamuel Rudolf Maranatha JulioÎncă nu există evaluări
- Boards SyllabusDocument14 paginiBoards Syllabus2012Încă nu există evaluări
- Boards SyllabusDocument14 paginiBoards Syllabus2012Încă nu există evaluări
- PCAP UpdatesDocument60 paginiPCAP Updates2012Încă nu există evaluări
- USMLEboardswhatworked 2008Document32 paginiUSMLEboardswhatworked 20082012Încă nu există evaluări
- General Recommendation ImmunizationDocument69 paginiGeneral Recommendation Immunization2012Încă nu există evaluări
- ADA Summary of Guidelines 2011Document7 paginiADA Summary of Guidelines 2011IffatNaeemÎncă nu există evaluări
- The Division of Plastic SurgeryDocument36 paginiThe Division of Plastic Surgery2012Încă nu există evaluări
- Fa Step 1 ScheduleDocument5 paginiFa Step 1 ScheduleDinesh DalviÎncă nu există evaluări
- Cancer Pain Relief Who 1998Document86 paginiCancer Pain Relief Who 19982012100% (1)
- Review Lectures Forlu6: Basic Eye Exam Common Opd Complaints Common Er Cases PharmacologyDocument110 paginiReview Lectures Forlu6: Basic Eye Exam Common Opd Complaints Common Er Cases Pharmacologyupmed2012block9Încă nu există evaluări
- SCOPING DOCUMENT For WHO Treatment Guidelines On Pain Related ToDocument10 paginiSCOPING DOCUMENT For WHO Treatment Guidelines On Pain Related To2012Încă nu există evaluări
- Diseases of The Anus Rev#1CDocument77 paginiDiseases of The Anus Rev#1C2012Încă nu există evaluări
- CEBM Levels of EvidenceDocument2 paginiCEBM Levels of Evidence2012100% (2)
- Pharma EvaluationDocument1 paginăPharma Evaluation2012Încă nu există evaluări
- Review of The Evidence For Herbal Medications and NutraceuticalsDocument5 paginiReview of The Evidence For Herbal Medications and Nutraceuticals2012Încă nu există evaluări
- Clin Tox Oral Vs IV ActylcysteineDocument19 paginiClin Tox Oral Vs IV Actylcysteine2012Încă nu există evaluări
- Glomerulonephritis Block A TransDocument7 paginiGlomerulonephritis Block A Trans2012Încă nu există evaluări
- CSAP Full 2002Document125 paginiCSAP Full 20022012Încă nu există evaluări
- Test Blueprint For Final Exam 2008-2009 For 75 PtsDocument3 paginiTest Blueprint For Final Exam 2008-2009 For 75 Pts2012Încă nu există evaluări
- Art of Med Trans Feb 28Document9 paginiArt of Med Trans Feb 282012Încă nu există evaluări
- Trans Pulmopatho ColoredDocument8 paginiTrans Pulmopatho Colored2012Încă nu există evaluări
- Patho Lab Trans - ButchDocument6 paginiPatho Lab Trans - Butch2012Încă nu există evaluări
- OS 214 - Renal Module - Imaging of The KUBDocument9 paginiOS 214 - Renal Module - Imaging of The KUB2012Încă nu există evaluări
- Organ Transplantation, Immunology and RejectionDocument2 paginiOrgan Transplantation, Immunology and Rejection2012Încă nu există evaluări
- Renal Patho Lab 2 PART 1 ColoredDocument8 paginiRenal Patho Lab 2 PART 1 Colored2012Încă nu există evaluări
- Trans Glomerularpatho FinalDocument16 paginiTrans Glomerularpatho Final2012100% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 434 OS 212 PictoTrans - Cutaneous SymptomatologyDocument51 pagini434 OS 212 PictoTrans - Cutaneous Symptomatology2012Încă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Reading Unit 9 CardiologyDocument4 paginiReading Unit 9 CardiologyChristian SilvaÎncă nu există evaluări
- Deep Vein Thrombosis: Carla C. Fernández Santos Universidad Central Del Caribe, Bayamón, PR Family MedicineDocument20 paginiDeep Vein Thrombosis: Carla C. Fernández Santos Universidad Central Del Caribe, Bayamón, PR Family MedicineCarla C. FernandezÎncă nu există evaluări
- The Lymphatics in Association With Sex HormonesDocument76 paginiThe Lymphatics in Association With Sex HormonesBryan ZeaÎncă nu există evaluări
- Midterms Group 5Document25 paginiMidterms Group 5Karina MadriagaÎncă nu există evaluări
- Left Ventricle Size, Mass, Volume and Function Reference RangesDocument33 paginiLeft Ventricle Size, Mass, Volume and Function Reference RangesEka Rahayu UtamiÎncă nu există evaluări
- Treating pedal edema in older adultsDocument2 paginiTreating pedal edema in older adultsIseth ISethÎncă nu există evaluări
- Weitzman Prize Cardiology Exam QuestionsDocument5 paginiWeitzman Prize Cardiology Exam QuestionsdanielmoffatÎncă nu există evaluări
- AZUR BrochureDocument4 paginiAZUR BrochureMayra Irene Osorio VásquezÎncă nu există evaluări
- Medical Terminology 2 Cardiovascular System Lesson 1Document3 paginiMedical Terminology 2 Cardiovascular System Lesson 1sotman58Încă nu există evaluări
- Eficacia Del FlowaveDocument6 paginiEficacia Del FlowaveLISFLOWERÎncă nu există evaluări
- Stroke-2004-Van Der Schaaf-1614-8 PDFDocument6 paginiStroke-2004-Van Der Schaaf-1614-8 PDFPalneuro UnsriÎncă nu există evaluări
- Hematoma Cerebral Intraparenquimatoso e Intraventricular Por Cocaína: Reporte de Un CasoDocument7 paginiHematoma Cerebral Intraparenquimatoso e Intraventricular Por Cocaína: Reporte de Un CasoCarolina GuzmánÎncă nu există evaluări
- Clinical Examination of Varicose VeinsDocument6 paginiClinical Examination of Varicose VeinsR.m. AndriyanÎncă nu există evaluări
- EmbolismDocument11 paginiEmbolismSubhrajyoti RoyÎncă nu există evaluări
- Perimount Theon: Carpentier-Edwards Mitral Pericardial BioprosthesisDocument4 paginiPerimount Theon: Carpentier-Edwards Mitral Pericardial BioprosthesisJose Miguel GonzalezÎncă nu există evaluări
- Vasculitis PPT NotesDocument14 paginiVasculitis PPT Noteshasanatiya41Încă nu există evaluări
- Physiology LE3 Samplex 2017BDocument8 paginiPhysiology LE3 Samplex 2017BAxel Alvaran100% (1)
- Innovative Lesson Plan.Document5 paginiInnovative Lesson Plan.MANOJÎncă nu există evaluări
- Iii. Hasil Dan PembahasanDocument10 paginiIii. Hasil Dan PembahasanHarditya FirdhausÎncă nu există evaluări
- Guiding Catheters in Coronary Agngioplasty: DR - KefelegnDocument64 paginiGuiding Catheters in Coronary Agngioplasty: DR - KefelegnerickÎncă nu există evaluări
- Hypertension (Clinical) Hadeel HlayelDocument133 paginiHypertension (Clinical) Hadeel Hlayeljana.alngÎncă nu există evaluări
- Introduction To The Cardiovascular SystemDocument22 paginiIntroduction To The Cardiovascular Systemwaqas_xsÎncă nu există evaluări
- Anatomy and PhysiologyDocument6 paginiAnatomy and PhysiologyJulianne B. Dela CruzÎncă nu există evaluări
- Pathogenesis of Atherosclerosis A Review: Imedpub JournalsDocument6 paginiPathogenesis of Atherosclerosis A Review: Imedpub JournalsHaydee RocaÎncă nu există evaluări
- Fundamentals of Body CT 5th EdDocument415 paginiFundamentals of Body CT 5th EdRuxandra TartaÎncă nu există evaluări
- CVS ExaminationDocument85 paginiCVS ExaminationPrasenjit DasÎncă nu există evaluări
- Transducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistDocument1 paginăTransducer Frequency - 205/305/5.0 MHZ: DR Satish Kumar Sharma Consultant CardiologistHappyÎncă nu există evaluări
- Cardiac DiseasesDocument8 paginiCardiac DiseasesTJ NgÎncă nu există evaluări
- Management of Pulmonary EdemaDocument42 paginiManagement of Pulmonary Edemaademato4real576Încă nu există evaluări
- Lesson-Proper of A Lesson PlanDocument2 paginiLesson-Proper of A Lesson PlanNhicolle DancelÎncă nu există evaluări