S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Success Criteria For Dental Implant - A Literature Review: Research ArticleDocument5 paginiSuccess Criteria For Dental Implant - A Literature Review: Research Articlehimanshu vadherÎncă nu există evaluări
- The Shoulderless Approach by TTDocument19 paginiThe Shoulderless Approach by TTMahmoud HeshamÎncă nu există evaluări
- Worn DentitionDocument8 paginiWorn DentitionHassan MoussaouiÎncă nu există evaluări
- Restoration Techniques and Marginal Overhang in Class II Composite Resin RestorationsDocument6 paginiRestoration Techniques and Marginal Overhang in Class II Composite Resin RestorationsCodrin TÎncă nu există evaluări
- Preparation Design and Considerations For Direct Posterior Composite Inlay:Onlay RestorationDocument7 paginiPreparation Design and Considerations For Direct Posterior Composite Inlay:Onlay RestorationAnonymous PqVoA059Încă nu există evaluări
- Efficacy of Transpalatal Arch As An Anchorage Rein PDFDocument7 paginiEfficacy of Transpalatal Arch As An Anchorage Rein PDFOana CostanÎncă nu există evaluări
- Maxillary Protraction Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental AcademyDocument121 paginiMaxillary Protraction Dr.M.M.varadharaja / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- Esthetic Rehabilitation of Worn Anterior Teeth With Thin Porcelain Laminate VeneersDocument17 paginiEsthetic Rehabilitation of Worn Anterior Teeth With Thin Porcelain Laminate VeneersJason LeeÎncă nu există evaluări
- Turner Nichol Scott 1991Document19 paginiTurner Nichol Scott 1991Virgi100% (1)
- Dentek Dental Guard User GuideDocument16 paginiDentek Dental Guard User GuideGreg JohnsonÎncă nu există evaluări
- Clinical Case Presentation Sample McqsDocument10 paginiClinical Case Presentation Sample McqsDr.yamini Nag Kantipudi100% (2)
- Porcelain: Composition and Characteristics of PorcelainDocument2 paginiPorcelain: Composition and Characteristics of PorcelainbigojiraÎncă nu există evaluări
- Cold-Welded Healing Cap A Unique Implant Complication and Its ManagementDocument5 paginiCold-Welded Healing Cap A Unique Implant Complication and Its ManagementdeepthiÎncă nu există evaluări
- Dental Anatomy QuestionsDocument16 paginiDental Anatomy QuestionsAmrit75% (12)
- Eur J Dent Zana LilaDocument8 paginiEur J Dent Zana LilaTien Li AnÎncă nu există evaluări
- Rinchuse 2006Document8 paginiRinchuse 2006jhon HanselÎncă nu există evaluări
- Troubleshooting and Management of Denture ProblemsDocument6 paginiTroubleshooting and Management of Denture ProblemsNur KamaliahÎncă nu există evaluări
- 2012 AAO Glossary - 0Document44 pagini2012 AAO Glossary - 0Lucia DueñasÎncă nu există evaluări
- History of Orthodontics PPDocument157 paginiHistory of Orthodontics PPAnant Jyoti100% (3)
- Food ImpactionDocument6 paginiFood ImpactionFaklina Juli100% (1)
- Mand. MolarsDocument15 paginiMand. MolarsMeera SÎncă nu există evaluări
- Neutral Zone Impression TechniqueDocument2 paginiNeutral Zone Impression Techniqueizeldien5870100% (2)
- Crown 2 QB: Put T&F. and Correct The False StatementDocument17 paginiCrown 2 QB: Put T&F. and Correct The False StatementMustafa SaßerÎncă nu există evaluări
- 6 Elements of Orofacial HarmonyDocument6 pagini6 Elements of Orofacial Harmonyjonathanza14Încă nu există evaluări
- Laser Gingival RetractionDocument3 paginiLaser Gingival RetractionCristobalVeraÎncă nu există evaluări
- Endodontics Principles and Practice (139 279)Document141 paginiEndodontics Principles and Practice (139 279)Daniel Ricardo Moreno HernandezÎncă nu există evaluări
- A Clinical Overview of Removable Prostheses - 2.impression Making For Partial DenturesDocument5 paginiA Clinical Overview of Removable Prostheses - 2.impression Making For Partial DenturesManea N. IonuțÎncă nu există evaluări
- David's ProjectDocument7 paginiDavid's Projectasulliv3Încă nu există evaluări
- Surgical-Orthodontic Treatment of Class I Malocclusion With Maxillary Vertical Excess - A Case ReportDocument7 paginiSurgical-Orthodontic Treatment of Class I Malocclusion With Maxillary Vertical Excess - A Case ReportFabian BarretoÎncă nu există evaluări
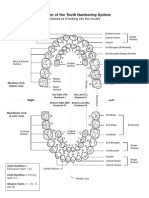
- Diagram of The Tooth Numbering SystemDocument1 paginăDiagram of The Tooth Numbering Systemsaleh900Încă nu există evaluări