S-ar putea să vă placă și
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationDe la EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationÎncă nu există evaluări
- Critical Appraisal of A Quasi-ExperimentalDocument10 paginiCritical Appraisal of A Quasi-Experimentallouie pilienÎncă nu există evaluări
- Joshua Ofori EssiamDocument9 paginiJoshua Ofori EssiamOfori EssiamÎncă nu există evaluări
- Doctor PT RelationshipDocument7 paginiDoctor PT RelationshipSanjeevan DeodharÎncă nu există evaluări
- Journal Article Critique Nursing 665Document5 paginiJournal Article Critique Nursing 665api-214213767Încă nu există evaluări
- Quantitative Article CritiqueDocument8 paginiQuantitative Article CritiqueGareth McKnightÎncă nu există evaluări
- Clinical Performance Assessments - PetrusaDocument37 paginiClinical Performance Assessments - Petrusaapi-3764755100% (1)
- Patient's Satisfaction With Perioperative Care: Development, Validation, and Application of A QuestionnaireDocument8 paginiPatient's Satisfaction With Perioperative Care: Development, Validation, and Application of A QuestionnaireHugo GutiérrezÎncă nu există evaluări
- Sample - Critical Review of ArticleDocument11 paginiSample - Critical Review of Articleacademicproffwritter100% (1)
- Centralization Versus Decentralization ADocument5 paginiCentralization Versus Decentralization AArjit AgarwalÎncă nu există evaluări
- Group SummeryDocument3 paginiGroup Summeryapi-525310113Încă nu există evaluări
- Evidenced Based Nursing PracticeDocument7 paginiEvidenced Based Nursing PracticeKim ViñasÎncă nu există evaluări
- Project ReportDocument41 paginiProject ReportAnoop PunathilÎncă nu există evaluări
- Research ForumDocument34 paginiResearch ForumJustine May GervacioÎncă nu există evaluări
- Appraisal of Evidence WorksheetsDocument10 paginiAppraisal of Evidence Worksheetsapi-577634408Încă nu există evaluări
- Managing Change Towards Bedside Shift ReportDocument12 paginiManaging Change Towards Bedside Shift Reportapi-438607141Încă nu există evaluări
- Validity, Reliability, and Generalizability in QualitativeDocument5 paginiValidity, Reliability, and Generalizability in Qualitativedan gzz100% (1)
- The Use of Patient Complaints To Drive QualityDocument8 paginiThe Use of Patient Complaints To Drive QualitysanaaÎncă nu există evaluări
- Professional Med J Q 2013 20 6 973 980Document8 paginiProfessional Med J Q 2013 20 6 973 980Vikram AripakaÎncă nu există evaluări
- ResearchDocument22 paginiResearchsheebaÎncă nu există evaluări
- Article ReviewDocument15 paginiArticle ReviewHamza Dawid HamidÎncă nu există evaluări
- Integrative Research of The LiteratureDocument14 paginiIntegrative Research of The Literatureapi-607378712Încă nu există evaluări
- Clinical Handover and Patient Safety Literature Review Report 2005Document5 paginiClinical Handover and Patient Safety Literature Review Report 2005gw163ckjÎncă nu există evaluări
- ResponseDocument2 paginiResponsekartikukulkarniÎncă nu există evaluări
- Patient Satisfaction DissertationDocument9 paginiPatient Satisfaction DissertationBuyCollegePapersSingapore100% (1)
- Patient Satisfaction As An Indicator of The Quality of Nursing CareDocument9 paginiPatient Satisfaction As An Indicator of The Quality of Nursing CareWILLIAM LOVE DIAN SAFITRIÎncă nu există evaluări
- Summary of Purposes and ObjectivesDocument19 paginiSummary of Purposes and Objectivesrodolfo opido100% (1)
- Nursing Care Quality 1Document11 paginiNursing Care Quality 1Nora100% (1)
- Patient's Satisfaction With Perioperative Care: Development, Validation, and Application of A QuestionnaireDocument8 paginiPatient's Satisfaction With Perioperative Care: Development, Validation, and Application of A QuestionnaireIda KatarinaÎncă nu există evaluări
- He U.S. Hospital System Suffers From ShortfallsDocument8 paginiHe U.S. Hospital System Suffers From Shortfallsjoy gorreÎncă nu există evaluări
- Impact - of - Hospital - Service - Quality - Dimensions - On - Customer Loyalty Final 23-12-12Document31 paginiImpact - of - Hospital - Service - Quality - Dimensions - On - Customer Loyalty Final 23-12-12badrinathÎncă nu există evaluări
- Reflective JournalsDocument19 paginiReflective JournalsisisvlvtÎncă nu există evaluări
- Doctor Patient Communication Literature ReviewDocument6 paginiDoctor Patient Communication Literature Reviewaflsvagfb100% (1)
- JournalDocument6 paginiJournalkhaiz_142989Încă nu există evaluări
- Patient Satisfaction With Nursing Care Quality and Patient Safety Culture in The Medical-Surgical UnitDocument10 paginiPatient Satisfaction With Nursing Care Quality and Patient Safety Culture in The Medical-Surgical UnitNurunnisa yrÎncă nu există evaluări
- Ethical Issues in Healthcare ManagementDocument44 paginiEthical Issues in Healthcare ManagementTravel with NiroÎncă nu există evaluări
- Customer Perception Towards Private HospitalsDocument29 paginiCustomer Perception Towards Private HospitalsBilal Ah Parray90% (10)
- Chapter IIDocument9 paginiChapter IICatherine R. FelipeÎncă nu există evaluări
- Chapter IIDocument9 paginiChapter IICatherine R. FelipeÎncă nu există evaluări
- Ethical Challenges in Qualitative Research: Examples From PracticeDocument12 paginiEthical Challenges in Qualitative Research: Examples From PracticecdxskierÎncă nu există evaluări
- Explore Adult Patients Opinions of Nursing Care in Medical-Surgical Wards PDFDocument8 paginiExplore Adult Patients Opinions of Nursing Care in Medical-Surgical Wards PDFnasimhsÎncă nu există evaluări
- Show PDFDocument4 paginiShow PDFalina breazuÎncă nu există evaluări
- Research Method and MeasurementsDocument9 paginiResearch Method and MeasurementsKaleta gebreÎncă nu există evaluări
- Cunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyDocument21 paginiCunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyMilton david Rios serratoÎncă nu există evaluări
- HR Action ResearchDocument7 paginiHR Action ResearchChristel DilleraÎncă nu există evaluări
- Barriball & While 1994 Collecting Data Using A Semi-Structured Interview JANDocument8 paginiBarriball & While 1994 Collecting Data Using A Semi-Structured Interview JANAnonymous HiWWDeIÎncă nu există evaluări
- A Grounded TheoryDocument15 paginiA Grounded TheorypicartmaÎncă nu există evaluări
- The Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryDocument15 paginiThe Effect of Structured Nursing Rounds On The Level Nursing Care Satisfaction of Patient in A Selected Tertiary Care Hospital, PuducherryIJAR JOURNALÎncă nu există evaluări
- Fountain 2016Document23 paginiFountain 2016Alfred RodÎncă nu există evaluări
- Health Education: Evidenced Based PracticesDocument58 paginiHealth Education: Evidenced Based PracticesChantal Raymonds90% (41)
- Qualitative Article CritiqueDocument9 paginiQualitative Article CritiqueJohn Smith100% (2)
- Related Literature and StudiesDocument12 paginiRelated Literature and StudiesYuuki Chitose (tai-kun)Încă nu există evaluări
- Ebp PosterDocument1 paginăEbp Posterapi-283540594Încă nu există evaluări
- Chapter 5Document42 paginiChapter 5Yuuki Chitose (tai-kun)Încă nu există evaluări
- Chapter 1Document11 paginiChapter 1Yuuki Chitose (tai-kun)Încă nu există evaluări
- The Use of Patient Complaints To Drive Quality Improvement: An Exploratory Study in TaiwanDocument7 paginiThe Use of Patient Complaints To Drive Quality Improvement: An Exploratory Study in TaiwanNurhafifa YusufÎncă nu există evaluări
- Articol StiintificDocument16 paginiArticol StiintificAndreea SanduÎncă nu există evaluări
- Effects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyDocument13 paginiEffects of Nursing Rounds: On Patients' Call Light Use, Satisfaction, and SafetyhanimozaghiÎncă nu există evaluări
- Negar and Eh 2014Document4 paginiNegar and Eh 2014vindhiÎncă nu există evaluări
- Quality of Post-Operative Nursing Care Among Patients Subjected To Cardiac SurgeryDocument3 paginiQuality of Post-Operative Nursing Care Among Patients Subjected To Cardiac Surgeryjilan Amer abdullahÎncă nu există evaluări
- Smashwords Book Marketing GuideDocument31 paginiSmashwords Book Marketing Guidekanikatekriwal126Încă nu există evaluări
- Presentation (India)Document42 paginiPresentation (India)kanikatekriwal126Încă nu există evaluări
- Chicago Travel GuideDocument54 paginiChicago Travel Guidekanikatekriwal126100% (2)
- 11 Evolution of Marketing Organization & Marketing AuditDocument38 pagini11 Evolution of Marketing Organization & Marketing Auditkanikatekriwal126Încă nu există evaluări
- The Greatest Love Poems Ever WrittenDocument146 paginiThe Greatest Love Poems Ever WrittenRobert CindreaÎncă nu există evaluări
- Business of Cross FitDocument11 paginiBusiness of Cross FitShah MilzanÎncă nu există evaluări
- Love Poems Erich FriedDocument29 paginiLove Poems Erich Friedgergberger0% (1)
- Module 10 - Marketing Best Practices - Publicview PDFDocument21 paginiModule 10 - Marketing Best Practices - Publicview PDFkanikatekriwal126Încă nu există evaluări
- Service Marketing 1Document40 paginiService Marketing 1kanikatekriwal126Încă nu există evaluări
- Icra Comments On Rbi'S Draft Guidelines For NBFCS: Background and OutlookDocument5 paginiIcra Comments On Rbi'S Draft Guidelines For NBFCS: Background and Outlookkanikatekriwal126Încă nu există evaluări
- PSSC Maths Statistics Project Handbook Eff08 PDFDocument19 paginiPSSC Maths Statistics Project Handbook Eff08 PDFkanikatekriwal126Încă nu există evaluări
- PTC12 - Sun IB1 - Jim Hayden PDFDocument14 paginiPTC12 - Sun IB1 - Jim Hayden PDFkanikatekriwal126Încă nu există evaluări
- Icra Comments On Rbi'S Draft Guidelines For NBFCS: Background and OutlookDocument5 paginiIcra Comments On Rbi'S Draft Guidelines For NBFCS: Background and Outlookkanikatekriwal126Încă nu există evaluări
- Global EconomyDocument93 paginiGlobal Economykanikatekriwal126Încă nu există evaluări
- Vodafone GroupDocument11 paginiVodafone GroupprasishereÎncă nu există evaluări
- Indias Telecom SectorDocument14 paginiIndias Telecom Sectoramitdce0178Încă nu există evaluări
- ShocksDocument19 paginiShocksapi-14433492Încă nu există evaluări
- Best Asian BankDocument3 paginiBest Asian Bankkanikatekriwal126Încă nu există evaluări
- Product Range Planning and SelectionDocument19 paginiProduct Range Planning and Selectionkanikatekriwal126Încă nu există evaluări
- Fund Flow1Document7 paginiFund Flow1kanikatekriwal126Încă nu există evaluări
- GP 4 Branding of Hospital ServiceDocument14 paginiGP 4 Branding of Hospital Servicekanikatekriwal126Încă nu există evaluări
- Cash FlowDocument3 paginiCash Flowkanikatekriwal126Încă nu există evaluări
- Psych - Nursing InterventionsDocument23 paginiPsych - Nursing Interventionsmarie100% (19)
- BeaconDocument22 paginiBeaconCatawba SecurityÎncă nu există evaluări
- EssaysDocument8 paginiEssaysDilini RajakarunaÎncă nu există evaluări
- Antipsychotic Long Acting InjectionsDocument7 paginiAntipsychotic Long Acting InjectionsVoNda AprilianiÎncă nu există evaluări
- Health and Social Care A Level Coursework CommunicationDocument5 paginiHealth and Social Care A Level Coursework Communicationafjwdkwmdbqegq100% (2)
- Robinson, Reiter (2007) - Behavioral Consultation and Primary Care - A Guide To Integrating ServicesDocument493 paginiRobinson, Reiter (2007) - Behavioral Consultation and Primary Care - A Guide To Integrating ServicesAna PierettiÎncă nu există evaluări
- Mental Health and Mental IllnessesDocument108 paginiMental Health and Mental IllnessesVictoria VellaÎncă nu există evaluări
- NCP - Activity IntoleranceDocument2 paginiNCP - Activity IntolerancePaolo Belleza92% (12)
- PhysicalDocument10 paginiPhysicalDay NavatoÎncă nu există evaluări
- Patient Education in Hospital-At-homeDocument12 paginiPatient Education in Hospital-At-homeIkramIzatÎncă nu există evaluări
- Rotarian Action Groups Annual Report enDocument32 paginiRotarian Action Groups Annual Report enAT&T XCUMPICHÎncă nu există evaluări
- Style Magazine Regional Digital Edition August 2011Document132 paginiStyle Magazine Regional Digital Edition August 2011StyleMediaGroup100% (1)
- The Benefits of Rehabilitation For Palliative Care PatientsDocument10 paginiThe Benefits of Rehabilitation For Palliative Care PatientsAriel SantosÎncă nu există evaluări
- Aisbisf-Cir-04 Dated 19.04.2022-Uniform Transfer Policy For Award Staff (2022)Document7 paginiAisbisf-Cir-04 Dated 19.04.2022-Uniform Transfer Policy For Award Staff (2022)Mahesh GhsÎncă nu există evaluări
- A Guide For Patients and Physicians: The Washington State Medical Marijuana ActDocument4 paginiA Guide For Patients and Physicians: The Washington State Medical Marijuana Actelioom100% (2)
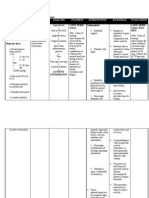
- Assessment Nursing Diagnoses Planning Implementation Rationale Evaluation Subjective Data: Short-Term GoalDocument2 paginiAssessment Nursing Diagnoses Planning Implementation Rationale Evaluation Subjective Data: Short-Term GoalMark oliver GonzalesÎncă nu există evaluări
- Alzheimer's Disease Fact Sheet: Symptoms DementiaDocument16 paginiAlzheimer's Disease Fact Sheet: Symptoms DementiaJovelyn Morales JosolÎncă nu există evaluări
- Regional Dementia ProgrammeDocument19 paginiRegional Dementia ProgrammeJonathon KingÎncă nu există evaluări
- Palliative Medicine and Supportive CareDocument12 paginiPalliative Medicine and Supportive CareKaren CárcamoÎncă nu există evaluări
- Benjamin 2010 Enhancing Building, Conversation, and Learning Through Caregiver-ChildDocument14 paginiBenjamin 2010 Enhancing Building, Conversation, and Learning Through Caregiver-ChildGyörgyi BallaÎncă nu există evaluări
- The Basics of Psychological First Aid (PFA)Document17 paginiThe Basics of Psychological First Aid (PFA)eduin pradaÎncă nu există evaluări
- Session 9 Spiritual and Psychosocial SupportDocument44 paginiSession 9 Spiritual and Psychosocial Supportstephen X-SILVERÎncă nu există evaluări
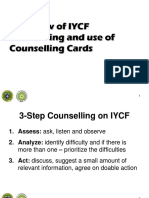
- IYCF Counselling Cards ChildFundPCADocument34 paginiIYCF Counselling Cards ChildFundPCAChris-Goldie LorezoÎncă nu există evaluări
- National Early Childhood CurriculumDocument72 paginiNational Early Childhood CurriculumEbiere Adeh100% (1)
- Tle 7 1ST Quarter ReviewerDocument13 paginiTle 7 1ST Quarter ReviewerRalph Louis RosarioÎncă nu există evaluări
- Au Pair Cover Letter ExampleDocument8 paginiAu Pair Cover Letter Examplewnfmbhsmd100% (1)
- Nursing-Associates-Proficiency-Standards 2Document30 paginiNursing-Associates-Proficiency-Standards 2SteveÎncă nu există evaluări
- Patient CounsellingDocument13 paginiPatient CounsellingAsfa IltamasÎncă nu există evaluări
- English 5-Q4-L16 ModuleDocument17 paginiEnglish 5-Q4-L16 ModuleMary Joy Rapadas100% (1)
- Unit Curriculum Map-Tle 7Document5 paginiUnit Curriculum Map-Tle 7ven bona100% (1)