S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
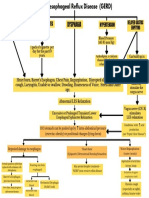
- Pathophysiology of Gastroesophageal Reflux (Gerd)Document1 paginăPathophysiology of Gastroesophageal Reflux (Gerd)Joville DorueloÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Presentation PathophysiologyDocument11 paginiPresentation PathophysiologyJade DeopidoÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Determination of Acid Neutralizing Capacity of Various Marketed Antacids in NepalDocument40 paginiDetermination of Acid Neutralizing Capacity of Various Marketed Antacids in NepalTshiva AryalÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Candida EsofagitisDocument5 paginiCandida EsofagitisVina IsmawatiÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- DR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHDocument47 paginiDR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHJennifer MrjÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- NPO GuidelinesDocument12 paginiNPO GuidelinesKi Tae JungÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- من جامعة الأردن PDFDocument266 paginiمن جامعة الأردن PDFyousefÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Pediatric Cervical Spine DeformityDocument52 paginiPediatric Cervical Spine DeformitySuresh MauryaÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- LIVER CHIRROSIS and GERED QUESTION AND ANSWERSDocument10 paginiLIVER CHIRROSIS and GERED QUESTION AND ANSWERSjess_nookieÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Ournal of Utrition Ollege: Journal of Nutrition CollegeDocument11 paginiOurnal of Utrition Ollege: Journal of Nutrition CollegeBunga HalimÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Acute Abdomen FinalDocument105 paginiAcute Abdomen FinalAizul AzmiÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- BISQDocument4 paginiBISQNanda Asyura RizkyaniÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Quiz 3Document7 paginiQuiz 3abezareljvenÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- GUJU Product List: WWW - Guju.co - KRDocument10 paginiGUJU Product List: WWW - Guju.co - KRsumanchyÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Gastroesophageal Reflux DiseaseDocument18 paginiGastroesophageal Reflux Diseasebrian3442Încă nu există evaluări
- Gastroesophageal Reflux Disease (Gastroenterology and Hepatology) PDFDocument408 paginiGastroesophageal Reflux Disease (Gastroenterology and Hepatology) PDFaab 1007Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Berklee Vocal Health For SingersDocument15 paginiBerklee Vocal Health For Singersrosalie_elena89% (9)
- Back To TopDocument2 paginiBack To Topangphone95Încă nu există evaluări
- Lewis CH 42 GIDocument13 paginiLewis CH 42 GIwismommyÎncă nu există evaluări
- Dexlansoprazole Vs Esomeprazole ERGEDocument12 paginiDexlansoprazole Vs Esomeprazole ERGELuis Felipe Gomez AndradeÎncă nu există evaluări
- Pediatrics-Case Presentation: - Sumanga, Juan Cheska Eunice ADocument62 paginiPediatrics-Case Presentation: - Sumanga, Juan Cheska Eunice ALhio Tuguegarao PcbÎncă nu există evaluări
- Drug StudyDocument2 paginiDrug Studycrianne_1180% (5)
- Brett Manning's Singing SuccessDocument18 paginiBrett Manning's Singing Successgabi50% (2)
- Nutrition - Eating and Singing - Musician Health and WellnessDocument4 paginiNutrition - Eating and Singing - Musician Health and WellnessOfori EbenezerÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Topic - Diaphragmatic HerniasDocument13 paginiTopic - Diaphragmatic HerniasOlga CerlatÎncă nu există evaluări
- Case Analysis 4 GERDDocument12 paginiCase Analysis 4 GERDCJ100% (1)
- 15 Natural Remedies For Heartburn & Severe Acid RefluxDocument60 pagini15 Natural Remedies For Heartburn & Severe Acid RefluxNISAR_786Încă nu există evaluări
- 18 Amla PittaDocument4 pagini18 Amla PittaAravind BharathiÎncă nu există evaluări
- Why Stomach Acid Is Essential For Our HealthDocument6 paginiWhy Stomach Acid Is Essential For Our HealthGabriel Turlac100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Digestive System KrvaDocument57 paginiDigestive System KrvaFercilyn MarbanÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)