S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
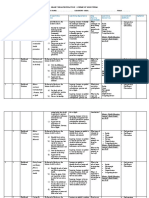
- Grade 7 SchemesDocument7 paginiGrade 7 SchemesMalesi SiemaÎncă nu există evaluări
- Yoli Acidity ReportDocument8 paginiYoli Acidity ReportTroy Dooly100% (1)
- Different Way of Food PreservationDocument22 paginiDifferent Way of Food PreservationMarynaire GallardoÎncă nu există evaluări
- International Ayurvedic Medical Journal April 2016Document198 paginiInternational Ayurvedic Medical Journal April 2016Safwan Shaikh50% (2)
- FInal PowerpointDocument77 paginiFInal PowerpointJacky ChanÎncă nu există evaluări
- Surprising Reason Why You May Need More Carbs PDFDocument14 paginiSurprising Reason Why You May Need More Carbs PDFrazvan rotaru100% (1)
- اول وحدتين من كونكت بلس 4 ماى فريندDocument74 paginiاول وحدتين من كونكت بلس 4 ماى فريندmido_20067581Încă nu există evaluări
- Final Reflection For EportfolioDocument2 paginiFinal Reflection For Eportfolioapi-241828006Încă nu există evaluări
- Judging CriteriaDocument2 paginiJudging CriteriaLeena BhaiÎncă nu există evaluări
- Final Exams - NUTRI EXAM FINALSDocument27 paginiFinal Exams - NUTRI EXAM FINALSJana Patricia JalovaÎncă nu există evaluări
- Prenatal Development Conception: - Nature NurtureDocument7 paginiPrenatal Development Conception: - Nature NurtureRomel Ciptoadi WijayaÎncă nu există evaluări
- Juicing For LifeDocument40 paginiJuicing For Lifeinfo_altenaÎncă nu există evaluări
- IELTS Writing Task 2 Practice 3Document2 paginiIELTS Writing Task 2 Practice 3ManpreetKalsiÎncă nu există evaluări
- MSC Chemistry Sem 4th - Lecture 1st VitaminDocument4 paginiMSC Chemistry Sem 4th - Lecture 1st VitaminArpitÎncă nu există evaluări
- ! 1 A 1 About A Absolute A MAX PYRAMID SUMMARIZED Posted by John Little UnderDocument9 pagini! 1 A 1 About A Absolute A MAX PYRAMID SUMMARIZED Posted by John Little UnderIt's Just Me100% (1)
- Successful Settling Suite IntroductionDocument5 paginiSuccessful Settling Suite Introductionpoojabanga81Încă nu există evaluări
- Module 3 VitaminsDocument9 paginiModule 3 VitaminsBig BrotherÎncă nu există evaluări
- Yoghurt and Sour Milk Products in Colombia - Analysis: Country Report - Sep 2020Document2 paginiYoghurt and Sour Milk Products in Colombia - Analysis: Country Report - Sep 2020Camila CajicaÎncă nu există evaluări
- Review of Related Literature: Chapter TwoDocument11 paginiReview of Related Literature: Chapter TwoLatifah Emam67% (3)
- Piping PloverDocument2 paginiPiping PloverConnecticut Wildlife Publication LibraryÎncă nu există evaluări
- Physical Education I Foundation of Fitness 1Document15 paginiPhysical Education I Foundation of Fitness 1Mary Sandylee TenaÎncă nu există evaluări
- Diagnostic Test in Mapeh 7Document3 paginiDiagnostic Test in Mapeh 7Chikahantayo TV100% (1)
- Grocery List (What You Can Eat During The First 3 Weeks - Yeast Fighting Diet)Document4 paginiGrocery List (What You Can Eat During The First 3 Weeks - Yeast Fighting Diet)peanutmilk100% (2)
- C 5 ProteinDocument20 paginiC 5 ProteinChristina HalderÎncă nu există evaluări
- Anaerobic Training: Prevention and Management of Exercise and Sport-Related InjuryDocument10 paginiAnaerobic Training: Prevention and Management of Exercise and Sport-Related InjuryKathy DamaulaoÎncă nu există evaluări
- Drug AnalysisDocument3 paginiDrug AnalysisAbby BorabienÎncă nu există evaluări
- The Food Pyramid and Nutrients Reading Comprehension Exercises - 106831Document3 paginiThe Food Pyramid and Nutrients Reading Comprehension Exercises - 106831Stephanie MorgendorfferÎncă nu există evaluări
- Product Design & RemediesDocument22 paginiProduct Design & RemediesaaaÎncă nu există evaluări
- The Bulking BlueprintDocument34 paginiThe Bulking BlueprintOmar ElouadÎncă nu există evaluări
- Theme 2: Thyroid Diseases: Study GoalsDocument9 paginiTheme 2: Thyroid Diseases: Study GoalsOlesyaÎncă nu există evaluări