S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chapter 91 - Diabetes MellitusDocument75 paginiChapter 91 - Diabetes MellitusPhúc NguyễnÎncă nu există evaluări
- Diabetes NCLEX QuestionsDocument22 paginiDiabetes NCLEX QuestionsGesta, Van Gerard T.Încă nu există evaluări
- Insulin Lispro: A Review of Its Use in The Management of Diabetes MellitusDocument28 paginiInsulin Lispro: A Review of Its Use in The Management of Diabetes Mellitusyunica simanjuntakÎncă nu există evaluări
- Diabetes and Fasting During RamadanDocument5 paginiDiabetes and Fasting During RamadanMila MoreiraÎncă nu există evaluări
- Clinical Guide to Diagnosis and Management of Diabetes MellitusDocument40 paginiClinical Guide to Diagnosis and Management of Diabetes MellitusTutde SedanaÎncă nu există evaluări
- Type 1 Diabetes MellitusDocument4 paginiType 1 Diabetes MellitusLaura Lhoeste100% (1)
- Ispad 2022Document477 paginiIspad 2022hakimadnenÎncă nu există evaluări
- Nilam Sari Effhallillah - 04021181924002 - Regular A 2019Document3 paginiNilam Sari Effhallillah - 04021181924002 - Regular A 2019Sekar Arum FamikatÎncă nu există evaluări
- Hyper - and HypoglycemiaDocument3 paginiHyper - and HypoglycemiaaerugiÎncă nu există evaluări
- DB 151028Document11 paginiDB 151028aminm23kÎncă nu există evaluări
- Present Scenario of Madhumeha Vis A Vis Diabetes Mellitus: Dr. R. ShripathiDocument26 paginiPresent Scenario of Madhumeha Vis A Vis Diabetes Mellitus: Dr. R. ShripathiSwagath NÎncă nu există evaluări
- Chapter 2Document2 paginiChapter 2Castro RicÎncă nu există evaluări
- Occupational Management of Workers With Diabetes MellitusDocument11 paginiOccupational Management of Workers With Diabetes Mellitusari gunawanÎncă nu există evaluări
- Gestational DiabetesDocument37 paginiGestational DiabetesSm BadruddozaÎncă nu există evaluări
- Diabetes MellitusDocument9 paginiDiabetes MellitusLorebellÎncă nu există evaluări
- Diabetes and PhysiotherapyDocument15 paginiDiabetes and Physiotherapyane2saÎncă nu există evaluări
- Physician and Patient Perception On Insulin TherapyDocument128 paginiPhysician and Patient Perception On Insulin TherapyEva GabrielÎncă nu există evaluări
- Nursing Analysis of HyperglycemiaDocument3 paginiNursing Analysis of HyperglycemiaDharylle Cariño100% (3)
- Self Instructional Training Methods To R 08c89fef PDFDocument6 paginiSelf Instructional Training Methods To R 08c89fef PDFIbu SaniyahÎncă nu există evaluări
- Group: 1. Dandi Rohadi 2. Gina Nurlaela 3. Intana Putri Meizira 4. Kurniawan Class 3A S1 KeperawatanDocument4 paginiGroup: 1. Dandi Rohadi 2. Gina Nurlaela 3. Intana Putri Meizira 4. Kurniawan Class 3A S1 KeperawatanDandiÎncă nu există evaluări
- Rencana Kebutuhan Reagen (Bahan Laboratorium) Puskesmas Penebel IDocument2 paginiRencana Kebutuhan Reagen (Bahan Laboratorium) Puskesmas Penebel IGustiAyuLilikRaiatiÎncă nu există evaluări
- Self-Monitoring of Blood Glucose Among Patients With Type I Diabetes Mellitus in Buraidah CityDocument7 paginiSelf-Monitoring of Blood Glucose Among Patients With Type I Diabetes Mellitus in Buraidah CityInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Drugs For Diabetes (Part 1)Document6 paginiDrugs For Diabetes (Part 1)حوراء عارف الموسويÎncă nu există evaluări
- 1123 Insulin ProtocolDocument7 pagini1123 Insulin ProtocolrosyadÎncă nu există evaluări
- 1644 4544 1 PB PDFDocument4 pagini1644 4544 1 PB PDFsitti nur vanesaÎncă nu există evaluări
- DM GerontikDocument15 paginiDM GerontikPuji Affan Dwi MiriyantoÎncă nu există evaluări
- Diabetes Mellitus Surgical PatientDocument33 paginiDiabetes Mellitus Surgical PatientGerald AndersonÎncă nu există evaluări
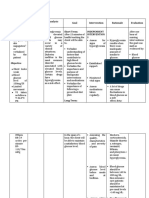
- ACTIVITY 1: Nursing Care PlanDocument4 paginiACTIVITY 1: Nursing Care PlanChelsea JardelezaÎncă nu există evaluări
- PSmarkup - Sheilatur Rohmah 161210037 PDFDocument67 paginiPSmarkup - Sheilatur Rohmah 161210037 PDFIrfan AndiÎncă nu există evaluări
- Konversi Insulin IV-sc 2Document12 paginiKonversi Insulin IV-sc 2Nurul Kamilah SadliÎncă nu există evaluări